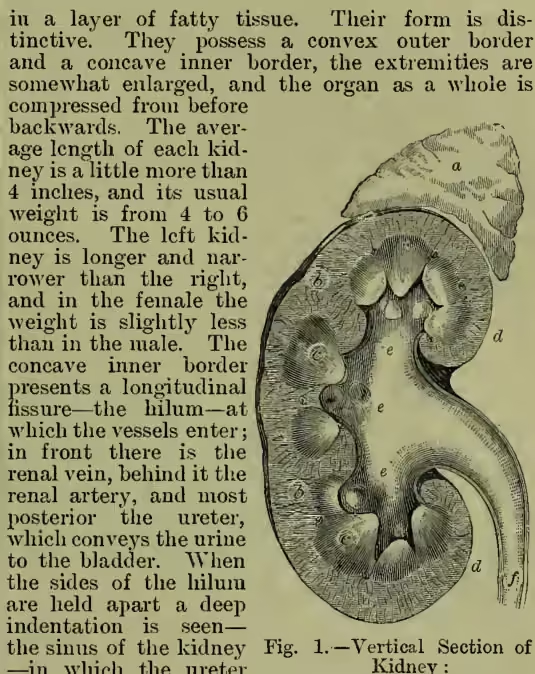
Kidneys, two glands having for their function the excretion of the urine. The human kidneys are situated in the region of the loins, one on each side of the spine, and are imbedded in a layer of fatty tissue. Their form is distinctive. They possess a convex outer border and a concave inner border, the extremities are somewhat enlarged, and the organ as a whole is compressed from before backwards. The average length of each kidney is a little more than 4 inches, and its usual weight is from 4 to 6 ounces. The left kidney is longer and narrower than the right, and in the female the weight is slightly less than in the male. The concave inner border presents a longitudinal fissure—the hilum—at which the vessels enter; in front there is the renal vein, behind it the renal artery, and most posterior the ureter, which conveys the urine to the bladder. When the sides of the hilum are held apart a deep indentation is seen—the sinus of the kidney—in which the ureter dilates to form a large sac, the pelvis of the kidney. Investing the kidney there is a fibrous coat—the tunica albuginea—which readily peels off from the substance of the gland to which it adheres by minute processes and fine blood-vessels. At the hilum it turns inwards, and becomes continuous with the sheaths of the vessels. Under cover of this capsule there is an incomplete layer of involuntary muscular fibre. The substance of the kidneys is dense, extremely friable, and of a deep red colour. On making a longitudinal section of the kidney from the convex outer border to the hilum it is seen to consist of two different substances, which are named, from their position, the external or cortical and the internal or medullary substance, arranged in pyramids with their apices towards the hilum.
The cortical substance forms by far the greater part of the gland, and sends numerous prolongations inwards between the pyramids of the medullary substance. It is soft, granular, and contains numerous minute red globular bodies diffused throughout it, which are called, from their discoverer, the Malpighian bodies. Its substance is made up of the uriniferous tubes, capillaries, lymphatics, and nerves, held together by an intermediate parenchymatous substance.
The medullary substance consists of pale reddish, conical masses, called the pyramids of Malpighi. They are usually about twelve in number, but vary from eight to eighteen, and their apices (the papillæ) point towards the hollow space (termed the sinus or pelvis) which occupies the interior of the gland. The medullary structure is firmer than the cortical, and instead of being granular presents a striated appearance, from its being composed of minute diverging tubes (the uriniferous tubes), which run in straight lines through this portion of the kidneys, after having run in a highly-convoluted course through the cortical portion. From the base of each pyramid streaks pass through the cortex, named medullary rays, and the portions of cortical substance between the rays are called the labyrinth of the cortex.
The cavity occupying the interior of the kidneys (the sinus or pelvis) is lined by mucous membrane, which, through the medium of the ureter, is continuous with that of the bladder, and which extends into the tissue of the kidneys, to line the uriniferous tubes. The mucous membrane forms a cup-like cavity around the termination of each pyramid, and the cavity, termed the calyx, receives the urine from the open terminations of the tubes, and conveys it towards the pelvis, from whence it passes down the ureter into the bladder.
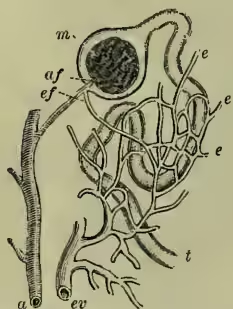
Each kidney is supplied with blood by a renal artery, a large trunk which comes off at right venous radicle, the efferent vessel, emerges from it close to the point at which the artery had entered. The Malpighian body itself, situated in the labyrinth, consists of a rounded bunch or tuft of capillaries, derived from the afferent and terminating in the efferent vessel, and enclosed in a clear and transparent capsule—the capsule of Bowman—lined with flattened epithelium. Each capsule is continuous with the uriniferous tube by a narrow neck.
It now remains to consider the respective functions of the Malpighian bodies and the tubes. From the researches of Bowman and others it appears that in animals in which the urinary excretion is passed in an almost solid form (as in birds and reptiles) the tufts are small and simple as compared with those in the kidneys of animals which (like man and most mammals) pass the urinary constituents dissolved in a large quantity of water. On these grounds, as well as from the fact that the anatomical arrangement of the tufts is well calculated to favour the escape of water from the blood, Bowman arrived at the conclusion that the function of the Malpighian bodies is to furnish the fluid portion (the water) of the urine. Recent observations tend to show that the saline ingredients of the urine are also excreted by Bowman's capsule. The arrangement of the convoluted portion of the tubes, with a capillary network on one side of their basement membrane, and secreting epithelial cells on the other, is the exact counterpart of the arrangement in other secreting glands, and there can be no doubt that the functions of the cells in the convoluted portion of the tubes is to separate from the blood the various organic con- stituents (urea, uric acid, creatinine, &c.) which collectively form the solid constituents of the urine. It does not necessarily follow that these secreting cells undergo rapid decay and renewal; it is more probable that they have the power of selecting certain materials from the blood, and of transmitting them, without the disintegration of their own structure, to the interior of the tube. The physical and chemical characters of the secretion yielded by the kidneys will be considered in the article URINE.
DISEASES OF THE KIDNEYS.—By far the most important are the group included under the general name of Bright's disease, which may be defined as comprising cases where structural changes in the kidneys, usually inflammatory, but without suppuration, lead to the presence of albumen in the urine. Dr Richard Bright published in 1827 researches showing that many cases of dropsy are attended by albuminuria on the one hand, and by marked changes in the kidneys on the other. His observations have been confirmed and extended by many subsequent observers; and it is now agreed that there are three distinct groups of cases, differing much in causation, symptoms, course, and post-mortem appearances, to which the above definition applies. These must be considered separately.
(1) Catarrhal or Parenchymatous Nephritis (inflammation of the kidneys).—In this form the inflammation affects chiefly the secreting structures of the kidney—i.e. the cells lining the tubules. The kidneys are at first much enlarged; in acute cases in the early stage redder than in health; in later stages and in chronic cases paler. If the duration of the disease is long, however, they may ultimately become much diminished in size, so as much to resemble, except in their paler colour, the kidneys in the cirrhotic form of Bright's disease. This disease may often be traced to exposure to cold; frequently complicates pregnancy; and occasionally occurs in connection with most of the eruptive fevers, but particularly scarlet fever, of which it is one of the most common and serious complications. In acute cases it sometimes begins with a rigor and elevation of temperature. Dropsy is almost always one of the earliest symptoms, and often appears first in the skin of the eyelids. Pain in the region of the kidneys, headache, and vomiting are usually present. The urine is scanty, often bloody, and contains albumen and tube-casts. Symptoms of Uremia (q.v.) often occur. In favourable cases complete recovery takes place in the course of a few weeks, all the symptoms gradually subsiding. Frequently, however, though the severer features of the case disappear, the urine continues to contain albumen, and the disease becomes chronic. Death may result from uræmia, from dropsical effusion, especially in the large serous cavities, frequently from the occurrence of some acute inflammation, particularly of lungs, pleura, or pericardium.
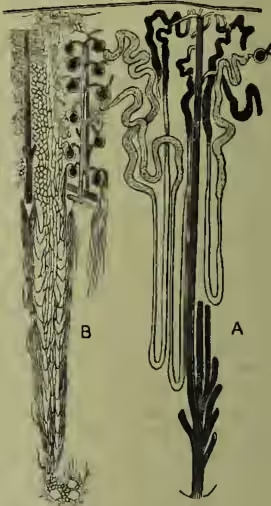
(From Macalister.)
(2) Cirrhosis of the Kidneys, or Interstitial Nephritis.—In this form the morbid process consists chiefly in chronic inflammation of the connective tissue of the kidney, which leads to destruction of the tubules and glomeruli by cicatricial contraction. In advanced cases the kidneys are much diminished in size, rough and nodular on the surface, and red in colour. This disease is often traceable to gout, either inherited or acquired, or to chronic lead-poisoning. It is rare before the age of thirty, most common after forty or forty-five. The chief feature of this affection is its extremely chronic and insidious nature, which is so marked that it is almost always for some secondary result of the disease that the patient seeks medical advice, and not for symptoms directly referable to the kidneys. The earliest symptom is usually an increase in the quantity of urine, which contains albumen only in small quantities, and may sometimes be quite free from it. Hypertrophy of the heart, with a hard pulse, is one of the most constant features of the disease; and in many cases symptoms due to heart affections are the first which excite the patient's alarm. Persistent headache, unaccountable vomiting or diarrhoea, failure of sight owing to albuminuric retinitis, simple debility, symptoms of uræmic poisoning, cerebral hæmorrhage (apoplexy), or the occurrence of acute inflammation of some internal organ—all these are among the occurrences which may lead to the discovery of this singularly insidious disease. It frequently becomes complicated by addition of inflammation of the kidney tubules (above described) to the primary process, and the symptoms are modified accordingly.
(3) Waxy or Lardaceous Degeneration of the Kidney.—As when this degenerative process appears in other organs, the smaller arteries and capillaries are first and most affected; later, other portions of the organ partake in the morbid process. But in the great majority of cases some degree of inflammation of the tubules is also present. Like waxy degeneration elsewhere, it can almost always be traced either to syphilis or to prolonged suppuration. The flow of urine is generally increased in the early stage, and contains albumen. Dropsy is usually present, with some others of the symptoms enumerated above as characteristic of the first form of Bright's disease. But in general the symptoms are rather variable, and could hardly lead to the recognition of the condition present apart from the clue given by the previous history of the case and the occurrence of signs of waxy disease in other organs. In acute cases (first form) prompt and active treatment is necessary, and is often signally successful. Confinement to bed between blankets, light diet, mainly or exclusively of milk, and the production of very free action of the skin and bowels are usually the chief points to be attended to. In the most severe cases wet-cupping or bleeding from the arm is sometimes required. Extreme care is necessary till perfect recovery has taken place. In chronic cases warm clothing, with attention to the action of the skin, strict regulation of the diet, avoidance of alcohol, and where possible removal to a warm climate during the cold season can do much to keep the disease in check. Experience has shown that under favourable conditions the course of the disease may be much more gradual than was generally believed by physicians thirty years ago.
Albuminuria without Bright's disease may occur in the course of fevers, in heart disease, and many other morbid conditions. It is now believed by most observers, though the subject is still under discussion, that it may also be present without any actual disease. Hæmoglobinuria (impregnation of the urine with the colouring matter of the blood) is a troublesome, but, except in the case of infants, not a dangerous disease. Hematuria (blood in the urine) is indicative of disease in some part of the urinary passages; but it is often difficult to be certain what portion is at fault. Besides Bright's disease, the most common condition leading to it is stone in the kidney or bladder. For Glycosuria (sugar in the urine) and Polyuria (increase in the quantity of urine), see DIABETES.
Stone in the Kidney.—The symptoms attending the passage of a stone from the kidney to the bladder have already been described (see CALCULUS); but it not infrequently happens that a stone formed in the kidney remains there, or, though it enters the ureter, fails to escape, blocking it and preventing the discharge of urine from that kidney. In either case the symptoms are often somewhat obscure and difficult to trace to their true cause. When the stone remains in the kidney blood generally appears from time to time in the urine, and there is persistent pain in the loin, often aggravated by such movements as the jolting of a carriage. Medicinal and dietetic treatment may often prevent the formation of fresh stones, where one has been discharged; and sometimes even seems to lead to the removal by solution of a stone from the kidney. Operation has frequently been resorted to during recent years for the removal of a stone from the kidney, and has in some cases relieved the symptoms, even when no stone has been discovered. When a stone becomes impacted in the ureter the kidney is gradually destroyed, and either atrophies or becomes converted into a large sac containing fluid. The remaining kidney generally becomes enlarged, and carries on the function of excretion: but if its ureter subsequently becomes obstructed in the same way death rapidly ensues.
Suppurative inflammation of the kidney may occur in the course of pyæmia, but usually results from disease of the lower urinary passages (bladder or urethra, hence often called surgical kidney), and is a very fatal disease. The kidneys may become the seat of tubercular disease, of malignant tumours, of hydatid cysts. But none of these conditions are of common occurrence.
Floating or Movable Kidney.—One kidney, more rarely both, may have its attachments to the posterior wall of the abdomen so loosened and elongated that it can move about in the abdominal cavity, somewhat as the intestines normally do. This condition is much more common in women than in men, and may either produce no symptoms, or lead to great discomfort and distress. In the latter case it is usually possible so to adapt a bandage and pad as to restrict the movements of the organ and to relieve the symptoms.