Knee, the articulation between the femur or thigh-bone, above, and the tibia or shin-bone, below. A third bone, the patella, or knee-cap, also enters into the structure of this joint anteriorly. The articular surfaces of these bones are covered with cartilage, and connected together by ligaments, some of which invest the joint and lie external to it, while others occupy its interior. The synovial membrane is the largest in the body. It lines the investing ligament, and is prolonged on the front of the femur above the articular surface, covers certain of the ligaments in the interior of the joint, and forms folds on a large cushion of fat placed between the tibia and patella.
The most important of the external ligaments are the anterior or Ligamentum Patellæ, which is in reality that portion of the Quadriceps Extensor Cruris which is continued from the knee-cap to the tubercle of the tibia; one internal and two external lateral ligaments; a posterior ligament; and a capsular ligament, which surrounds the joint in the
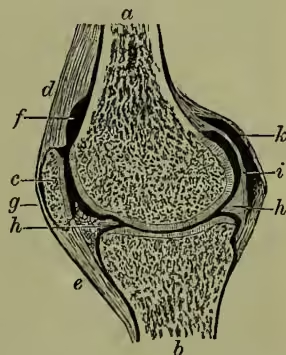
intervals left by the preceding ligaments. The positions of these ligaments are sufficiently indicated by their names. Of the internal ligaments the two crucial, so called because they cross one another, are the most important. The external and internal semilunar cartilages are usually placed amongst the internal ligaments; they are two crescentic plates of fibro-cartilage. The convex border of each cartilage is thick; the concave free border is thin. Each cartilage covers nearly the marginal two-thirds of the corresponding articular surface of the tibia, and by its form deepens these surfaces for firmer articulation with the condyles of the femur.
The chief movements of this joint are those of a hinge-joint—namely, flexion and extension; but it is also capable of slight rotatory motion when the knee is half-flexed. During flexion the articular surfaces of the tibia glide backwards upon the condyles of the femur; while in extension they glide forwards. The whole range of motion of this joint, from extreme flexion to extreme extension, is about 135°. Judging from its articular surfaces, which have comparatively little adaptation for each other, it might be inferred that this was a weak and insecure joint; and yet it is very rarely dislocated. Its real strength depends on the large size of the articular ends of the bones, on the number and strength of the ligaments, and on the powerful muscles and fasciae by which it is invested. See JOINTS, where also the excision of the knee-joint is discussed.
The KNEE-CAP, or PATELLA, is a Sesamoid Bone (q.v.), developed in the single tendon of the rectus, crureus, vastus externus, and vastus internus muscles—the great quadriceps extensor muscle of the leg. It is heart-shaped in form, the broad end being directed upwards, and the apex downwards. The anterior or external surface is convex, perforated by small apertures for the entrance of vessels, and marked by rough longitudinal striæ; the posterior or internal surface is smooth and divided into two facets by a vertical ridge, which corresponds and fits into the groove on the lower articulating surface of the femur or thigh-bone, while the two facets (of which the outer is the broader and deeper) correspond to the articular surface of the two condyles.
This bone is liable both to dislocation and fracture. Dislocation may occur either inwards or outwards; but it is most frequent in the outward direction. The displacement may be caused either by mechanical violence, or by too sudden contraction of the extensor muscles in whose conjoined tendon it lies; and is most liable to occur in knock-kneed, flabby persons. Except in one rare variety, the dislocation is capable of being reduced without any difficulty. Fracture of the patella may, like dislocation, be caused either by muscular action or by mechanical violence.
Fracture by violent muscular action, as when a person in danger of falling forwards attempts to recover himself by throwing the body backwards, is the more common of the two forms. The treatment consists in relaxing the opposing muscles by raising the trunk, and slightly elevating the limb, which should be kept in a straight position. In consequence of the great difficulty of bringing the broken surfaces into exact apposition it is very difficult to obtain bony reunion of the parts, and the case generally results either in mere ligamentous union or in no true union at all.