Larynx (Gr. larynx) is the organ of voice, and plays an important part in the respiratory process, as all air passing either to or from the lungs must pass through it. It is a complex piece of mechanism, resembling a box composed of pieces of cartilage which are capable of executing movements, and enclosing the vocal cords by which phonation is produced. The larynx is situated between the trachea, or windpipe, and the base of the tongue, it forms a considerable projection (especially in men); it opens superiorly into the pharynx, or throat, and inferiorly into the windpipe. The principal cartilages of which the skeleton of the larynx is composed are five in number—viz. the thyroid and cricoid cartilages, the epiglottis, and the two arytenoid cartilages.
The thyroid (Gr., 'shield-like') consists of two square plates of cartilage united in front at an acute angle, which forms the projection commonly known as the pomum Adami, or Adam's apple. Each of these plates is prolonged at the upper and lower posterior corners. The thy- roid cartilage forms almost the whole of the anterior and lateral walls of the larynx. The cricoid (Gr., 'ring-like') cartilage is a ring the lower margin of which is parallel to the first ring of the trachea, and to the last-named it is united by fibrous membrane. Its upper border is connected in front with the lower border of the thyroid cartilage by a thick yellow fibrous tissue. It presents two articular surfaces on either side—viz. a lower, which articulates with the inferior cornu of the thyroid cartilage, and an upper, which is oval in form, and supports an arytenoid cartilage. The arytenoid (Gr., 'ladle-like') cartilages are pyramidal bodies resting on the oval articular surfaces at the upper and posterior part of the cricoid cartilage.
When in situ they present a concave posterior surface. From their connection with the vocal cords, and from their great mobility as compared with the two larger cartilages, the arytenoids play a very important part in the mechanism of the larynx. The epiglottis is a very flexible cartilaginous valve (fig. 1, f), situated at the base of the tongue, and covering the opening of the larynx. Its direction is vertical, except during deglutition, when it becomes horizontal. It is attached inferi-
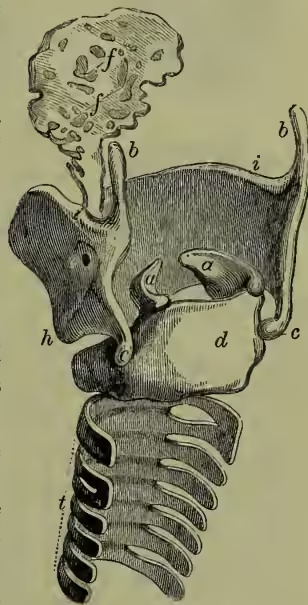
Cartilages of larynx and epiglottis, and upper rings of trachea, seen from behind: a, arytenoid cartilages; b, superior cornu of thyroid cartilage; c, its inferior cornu; d, posterior surface of cricoid; f, epiglottis, with its perforations; i, upper margin of thyroid; h, its left inferior tubercle; t, trachea. only by a kind of pedicle to the angle of the thyroid cartilage. Upon removing the investing mucous membrane the cartilage is found to be perforated by numerous foramina. Each perforation admits some fasciculi, of yellow, elastic, ligamentous tissue, which expands on its anterior aspect, and secures the return of the epiglottis to its vertical position, independently of any muscular action. Such is the skeleton of the larynx, hanging as it does from the hyoid bone, with which it is connected by the thyro-hyoid ligament and certain muscles.
The various cartilages which have been described are connected with one another by ligaments, the chief of which are those known as the true and false vocal cords. In their quiescent state the former do not lie parallel to each other, but converge from behind forwards. The length of the vocal cords is greater in the adult male than in the adult female, in the ratio of three to two. In infancy they are very short, and increase regularly from that period to the age of puberty. The mucous membrane of the larynx is part of the extensive respiratory tract, and is remarkable for its extreme sensibility. The length of the chink or aperture of the glottis, which is directed horizontally from before backwards, varies, like the severe form, which is fortunately rare, commences with a chill, which is followed by fever, with a full strong pulse, a hot skin, and a flushed face. There is also soreness of the throat, hoarseness of the voice, great difficulty in swallowing, and a feeling of extreme constriction of the larynx. There is a painful stridulous cough, but only a little mucus is ejected. Great difficulty in breathing occurs in severe cases, the act of inspiration being prolonged, and wheezing results, in consequence of the swollen membrane of the glottis impeding the entrance of air. On examining the larynx, the epiglottis is observed to be of a bright red colour, erect, and may be so much swollen as not to be able to descend, and may close the glottis during deglutition; the other parts of the larynx are seen to be more or less swollen according to the severity of the case. The patient may exhibit symptoms of great anxiety and distress; his lips may become blue, his face of a livid paleness, his pulse irregular and very feeble, and at length he may sink into a drowsy state, often preceded by delirium, and quickly followed by death. The disease is very rapid, ending, when fatal, in three or four days, and occasionally in less than one day. Although we have here described what may occur in exceptionally severe cases, acute laryngitis rarely passes beyond hoarseness, a feeling of constriction, slight feverishness associated with cough and marked hoarseness.
Laryngitis is most commonly due to exposure to cold; but the inflammation rarely reaches a dangerous height in these cases. The dangerous forms are usually the result of injury (e.g. swallowing boiling or corrosive substances); or they may be a secondary result of ulceration, or due to infection, such as erysipelas. In simple cases confinement to a warm room, with soothing steam inhalations, will, if the voice be rested, usually effect a cure. In severe cases sucking ice, leeching, scarification of the swollen parts, and even tracheotomy may be necessary. In persons who use the voice much the affection is apt to become chronic, or indeed to be chronic from the beginning without the supervision of an acute attack. Laryngotomy is discussed at TRACHEOTOMY.
Ulceration may occur in phthisis, syphilis, lupus, and after typhoid fever. Cancer of the larynx may lead to ulceration, but the primary disease constitutes a tumour. Innocent growths are also met with, the more common varieties being papillomata (warts) and fibromata. Paralysis of the laryngeal muscles may involve those muscles only which close the glottis, in which case the affection is often due to hysteria and easily cured. Paralysis of the muscles which open the glottis or affecting all the muscles is usually due to some grave disease of the nervous system, chest, or throat, and is often incurable. The treatment must depend upon the condition discovered by laryngoscopic examination in each case.
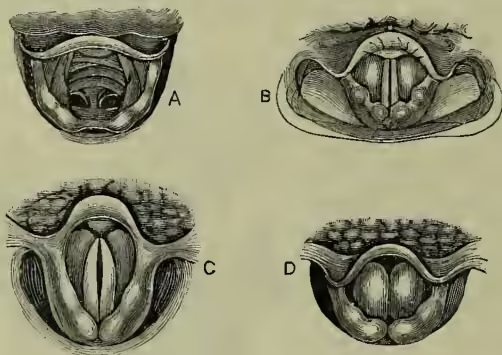
THE LARYNGOSCOPE.—Although successful attempts had been previously made by Garcia to explore the recesses of the larynx by means of a reflecting mirror, it was not until two German physiologists, Türk and Czermak, took up the subject, in 1857 and 1858, that the great importance of laryngoscopy was first generally recognised. The laryngoscope is a small mirror placed on a stalk attached to its margin, at an angle of from to , the stalk being about six inches in length. The mouthpiece of a large reflector, with a central opening through which the observer looks, is held between the molar teeth; or, what is better, the reflector may be attached to a spectacle frame or forehead band by a stiffly working ball-and-socket joint. The rays of the sun or of a good lamp are concentrated by means of this vocal cords, until the period of puberty, when its length, in the male, undergoes a sudden development, while in the female it remains stationary. In the adult male it is about eleven lines in length.
The larynx is provided with two sets of muscles: the extrinsic, by which the whole organ is elevated or depressed, and the intrinsic, which regulate the movements of the various segments of the organ in relation to one another. By the action of these latter muscles, aided, in some cases, by the extrinsic muscles, the tension of the vocal cords may be increased or diminished, and the size of the opening of the glottis regulated at will (see VOICE). The nerves of the larynx are derived from the superior and inferior laryngeal branches of the pneumogastric or vagus nerve.
That the larynx is the organ of voice is easily proved. Thus, alteration in the mucous membrane covering the vocal cords causes hoarseness or other change of voice; ulceration of the vocal cords destroys or injures the voice; opening the trachea below the vocal cords, or section of the inferior laryngeal nerves, destroys the voice; and sounds like those of the voice may be produced by experiments on the dead larynx.
DISEASES OF THE LARYNX.—Laryngitis, or inflammation of the larynx, may be either an acute or a chronic affection. Acute laryngitis, in its more reflector on the laryngeal mirror, which is placed against the soft palate and uvula. The laryngeal mirror, previously warmed, and introduced with the right hand, which rests by two fingers on the jaw, is maintained at such an inclination that it throws the light downwards and illuminates the parts to be examined, while at the same time it reflects the images of these parts into the eye of the observer through the central opening of the reflector. By this means we can look through the larynx into the trachea or windpipe, and can see the actual position of small tumours, ulcers, &c., whose existence would otherwise have been at most only suspected; and the precision and accuracy of diagnosis to which we can thus attain enable us to employ rational means of local treatment to an extent that was quite impossible before the introduction of laryngoscopy. It is also possible to illuminate the larynx by throwing a powerful and concentrated light upon the front of the throat, and introducing a mirror into the dark mouth (Durchleuchtung of German physicians).