Shoulder-joint, an enarthrodial or ball-and-socket joint. The bones entering into its formation are the humerus or arm-bone (see ARM) and the scapula or shoulder-blade. The former has already been described: the latter is a flat triangular bone which is indirectly attached to the trunk by articulation with the clavicle. When the arm hangs by the side the scapula covers the ribs posteriorly from the second to the seventh or eighth inclusive. It presents a posterior surface or dorsum, an anterior surface or venter, three borders, three angles, and certain outstanding processes.
The figure represents a posterior view of the scapula. It is divided into two unequal parts, the supra-spinous fossa (1) and the infra-spinous fossa (2), by the spine (10), a crest of bone commencing at a smooth triangular surface (11) on the internal border, and running across towards the upper part of the neck of the scapula (8), after which it alters its direction, and projects forwards so as to form a lofty arch, known as the acromion process (12), which overhangs the glenoid cavity (6), or receptacle for the head of the humerus. The acromion obviously serves to protect the shoulder-joint, as well as to give great leverage to the deltoid muscle which raises the arm. From the upper part of the neck (8) there proceeds a curved projection termed the coracoid process; it is about 2 inches long, and gives attachments to several muscles. The upper border of the scapula presents a notch (4), which in the recent state is bridged over by a ligament, and gives passage to the supra-scapular nerve.
The large globular head of the humerus is received into the shallow glenoid cavity of the scapula, an arrangement by which extreme freedom of movement is obtained, while the apparent insecurity of the joint is guarded against by the strong ligaments and tendons which surround it, and above by the arched vault formed by the under surface of the acromion process. As in movable joints generally, the articular surfaces are covered with cartilage, and there is a synovial membrane which lines the interior of the joint. The most important connecting medium between the two bones is the capsular ligament.
The shoulder-joint exhibits the following varieties of motion: (1) flexion, to a great extent; (2) extension, in a much more limited degree; (3) adduction, in an oblique direction, forwards and inwards; (4) abduction very freely; (5) circumduction; and (6) rotation slightly.
The morbid affections of the shoulder-joint may be divided into those arising from disease and those dependent on an accident. The most common diseases are acute and chronic inflammation of the joint, which often terminate in its ankylosis or immobility. The principal accidents are fractures and dislocations. There may be fracture (1) of the acromion process, or (2) of the coracoid process; (3) of the coracoid process, or (4) of the superior extremity of the humerus; or two or more of these accidents may be associated. Again, the head of the humerus may be dislocated from the glenoid cavity as the
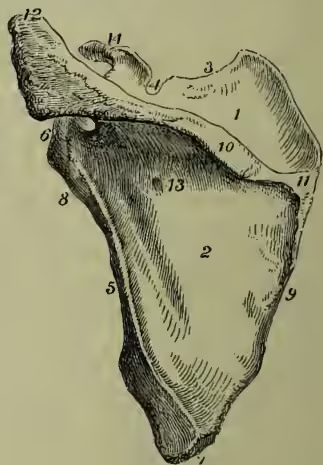
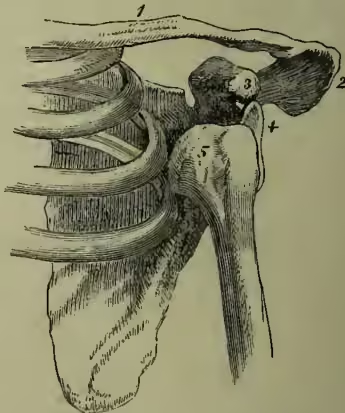
The parts designated by the figures 1, 2, 4, 6, 8, 10, 11, 12 are sufficiently described in the text; 3 is the superior border; 5, the external or axillary border; 7, the inferior angle; 9, the internal or vertebral border; 12, the acromion process; 13, one of the nutrient foramina; 14, the coracoid process. 1, the clavicle; 2, the acromion process; 3, the coracoid process; 4, the glenoid cavity; 5, the head of the humerus lying in the axilla. result of accident in three different directions—viz. (1) downwards and inwards into the axilla, which is by far the most common form; (2) forwards and inwards; and (3) backwards on the infra-spinous fossa, or the dorsum of the scapula. The first of these varieties is of very common occurrence, and everybody should know how to recognise, and even (in an emergency) to treat it. The bones are in the position shown in the figure; the arm is lengthened; a hollow may be felt under the acromion, where the head of the bone ought to be; the shoulder is flattened; the elbow sticks out from the side, and cannot be made to touch the ribs; and the head of the bone can be felt if the limb be raised, although such an attempt causes great pain and weakness. The methods of treating such a case are discussed at DISLOCATION. The scapula may also be fractured in any of its parts as the result of direct violence, and its inferior angle may slip from its natural position.