Arteries (Gr. artēria, probably from air-ein, 'to raise,' but by some connected with aēr, 'air,' from the old idea that these tubes were air-carriers, since after death they are generally found empty), the vessels through which the blood passes from the heart to the tissues. The structure of an arterial tube is very complex, and a section of it may be roughly subdivided into three layers, called the coats of the artery: an external, consisting of interlacing bundles of fibrous tissue mixed with elastic fibres, which in large vessels such as the aorta are gathered together to form an elastic layer; a middle, which is muscular, contractile, and brittle, the fibres being arranged in a circular direction; an internal, also brittle, the free surface being smooth and formed of a single layer of endothelial cells. External to these cells there is a layer of delicate connective tissue, outside which there is the elastic layer constituting the bulk of the inner coat, and distinguished by numerous perforations, causing its fenestrated appearance. The tube is also enveloped in cellular tissue, termed the sheath of the artery. When an
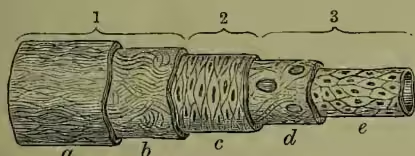
| 1. External coat | { | a, fibrous. |
| b, elastic. | ||
| 2. Middle coat | { | c, muscular. |
| d, elastic. | ||
| 3. Internal coat | { | e, endothelial. |
artery is wounded by a sharp instrument, the effect varies with the direction of the cut. Thus, if longitudinal, the edges may not separate, and the wound may heal without much bleeding; if oblique or transverse, the edges gape; and a nearly circular orifice allows of a profuse hemorrhage. If the artery be completely divided, its walls do not collapse like those of a vein, but pass through certain changes provided by nature to prevent fatal bleeding. The cut orifice contracts, and also retracts into its cellular sheath; this checks the flow of blood, a clot of which shortly forms on the outer side; then another forms inside the vessel; and together, they stem the flow, till the cut edges of the artery have time to throw out lymph (see ADHESION), and heal as wounds of other tissues. When an artery is compressed by a ligature, the brittle inner and middle coats crack and curl inwards. The interior of the vessel becomes filled with a clot which extends as far as the nearest collateral branch. Gradually the clot is absorbed and fibrous tissue deposited in its place, the result being that this part of the artery is entirely obliterated. See BLEEDING.
The arteries of the human body consist of two groups—those belonging to the lesser or pulmonic circulation, and those belonging to the greater or systemic circulation. All the offsets of the latter group are branches, more or less direct, of the aorta. As each main trunk passes into a portion of the body, it divides into two principal divisions: one, which breaks up into branches for the supply of the tissues in the vicinity—the artery of supply; and another, which passes almost branchless to supply the parts beyond—the artery of transmission. These, however, anastomose freely (see ANASTOMOSIS), so that the distant tissues are not solely dependent for their supply on only one arterial trunk. Thus the femoral artery divides in the groin into the profunda or deep femoral, to supply the thigh, and the superficial femoral, to supply the leg below the knee. Again, the common carotid divides into the external carotid, to supply the neck and head, and the internal carotid, to supply the brain. Although arteries have generally the same distribution or arrangement of branches, they frequently vary, and thereby are apt to puzzle a superficial anatomist. Some of the varieties are so common that it becomes difficult to decide which is normal. These peculiarities are often found as constant forms among lower animals, but in many cases they may be due simply to enlargement or diminution of vessels already existing. The principal arteries will be considered under their distinctive names, as at
Aorta (q.v.); and see CIRCULATION, BLOOD, HEART, VEIN.
DISEASES OF ARTERIES.—Arteries, like other organs of the body, are liable to acute inflammation (Arteritis); but this rarely occurs except as a consequence of inflammation in the neighbourhood of the vessel, or of obstruction of its tube (see below). By far the most common and important disease affecting arteries is Atheroma (from Gr. athērē, meal). Atheroma is commonly a disease of advanced life, but may be found at any age. Its occurrence is favoured by any cause which produces greatly increased arterial pressure (occupations or amusements involving very great physical exertion, excessive use of alcohol), probably also by syphilis. It commences with a chronic inflammation, with greatly increased formation of cells in the outer layers of the inner coat of the arteries, perhaps also in the middle coat. This infiltration causes destruction of the natural tissues of these coats, and consequent loss of elasticity and contractility in the parts of the artery affected. The inflamed portions of tissue undergo fatty degeneration, and may either (a) become so softened as to be carried away by the blood-stream, or, more commonly, (b) become gradually calcified—i.e. converted into bony plates by the deposition in them of chalky matter. (a) A portion of the wall of an artery weakened in this way rarely becomes perforated, but frequently yields to the blood-pressure, becomes dilated, and forms an Aneurysm (q.v.). (b) Calcification is much commoner, especially in old people, and may frequently be recognised in the superficial arteries by the hard feel the vessel has under the finger.
Atheromatous deposit is at first attended with a narrowing of the calibre of the vessel, varying with the thickness of the deposit, and most marked at the points of bifurcation. Smaller arteries may be completely obliterated, whilst the larger arteries may be very much contracted. Thus the common iliac has been found to have its canal diminished by about one-half, and the great ascending branches of the arch of the aorta, the subclavian and carotid arteries, have been found very nearly closed. A later consequence of the same disease is dilatation of the vessel. The elasticity of the outer coats being insufficient to contract the artery after the distension produced by each contraction of the left ventricle of the heart, it remains distended during the relaxation of the ventricle, and thus slowly expands; the enlargement being most marked at parts where there is most obstruction to the blood-current, as, for example, in curved arteries. These changes have also an effect on the retractile power of the arteries. A healthy artery, if cut across, may shorten to the extent of an inch or more; but the retractile power is destroyed by the deposition of bony rings or plates. But although incapable of shortening, the arteries sometimes become abnormally lengthened, and consequently become not only dilated, but also tortuous. All these changes produce great interference with the normal circulation of the parts whose arteries are affected; and where the disease is advanced, a cause that would otherwise be trivial may lead to serious results—e.g. softening of the brain, gangrene of the limbs, &c.
Another condition involving much danger is this: an ossified artery loses the smoothness which the interior of the vessel ought to present, and from the displacement or cracking of a bony plate, there may be sharp rough projections exposed, to which the fibrin of the circulating blood may adhere. These little clots becoming detached, may be carried with the blood till they become arrested, and plug up an artery, thus presenting cases of embolism or Thrombosis (q.v.). Again, the relation of this disease to accidents and surgical operations on arteries is obvious. A blow or strain may rupture a diseased artery, when a healthy elastic vessel might have escaped injury. Such a slight movement as suddenly lifting the arm to the head, for the purpose of securing the hat in a sharp gale, has been known to be followed by aneurysm of the axillary artery (Syme). A ligature applied to any calcified artery is very apt to cause it to break, and the difficulty of securing such vessels is often very great. It is to this form of disease that most of the failures of operations for aneurysm are due.
Atheroma can be detected in the living subject only in its advanced stages, and its presence is often revealed by the occurrence of some secondary disease or symptom.
Another form of chronic inflammation of the arteries is met with in syphilis. It consists in a uniform thickening of the inner coat of the vessel, without the degenerative changes of atheroma, but with great diminution of its calibre, and consequent interference with the circulation. It is best seen and most important in the brain, where it often leads to softening.
Embolism is the name given to the obstruction of an artery by a plug carried to it from another part of the body. This may follow atheroma (see above), but is most commonly a consequence of the detachment of a mass of fibrin from a diseased heart. Any artery may be obstructed by embolism; the consequences are most serious in the brain, the retina, and the limbs. In the larger arteries of the brain, embolism causes symptoms and results very similar to Apoplexy (q.v.); in the retina, it causes sudden and often complete loss of vision (see EYE, Vol. IV. p. 513).
When the principal artery of one of the limbs is 'suddenly plugged in its higher part, a sensation of severe pain is commonly the immediate result of the accident. In some cases, the pain extends along the course of the vessel, which, though pulseless, is extremely tender; in others, the suffering is referred to some distant part of the limb, as, for instance, to the calf. Signs of a deficient circulation succeed, and they may amount to pallor, loss of temperature, numbness of the surface, or even to that torpor which is observed to precede the total death of a limb in certain cases of injuries of vessels.' Although Gangrene (q.v.) is always to be feared as the result of an obstructed artery of large size, it does not invariably follow; as a collateral circulation may be established, and the life of the limb may be thus saved. Very young persons will endure the obliteration of very large vessels without gangrene; and a case is on record in which 'all the main arteries of both upper extremities and of the left side of the neck were reduced to solid cords,' and yet no gangrene ensued. From the description of the symptoms, the nature of a case of sudden occlusion of a large artery by a plug may possibly be recognised, or at all events suspected, even by a non-professional observer. Medical aid must at once be sought. The early indications of treatment are to preserve the temperature of the part, to favour the establishment of a collateral circulation, to protect the limb from irritation or injury, to give nourishing blood-making food, and to relieve pain by the judicious use of opiates. The later treatment, if the affection is not checked, is that which is described in GANGRENE.