Teeth, hard bodies in the mouth, attached to the skeleton, but not forming part of it, and developed from the dermis or true skin. 'They present,' says Owen, 'many varieties as to number, size, form, structure, position, and mode of attachment, but are principally adapted for seizing, tearing, dividing, pounding, or grinding the food. In some species they are modified to serve as formidable weapons of offence and defence; in others, as aids in locomotion, means of anchorage, instruments for uprooting or cutting down trees, or for transport and working of building materials. They are characteristic of age and sex; and in man they have secondary relations, subservient to beauty and to speech. Teeth are always intimately related to the food and habits of the animal, and are therefore highly interesting to the physiologist; they form, for the same reason, important guides to the naturalist in the classification of animals.'
True teeth consist of one, two, or more tissues, differing in their chemical composition and in their microscopical appearances. 'Dentine,' which forms the body of the tooth, and 'cement,' which forms its outer crust, are always present; the third tissue, the 'enamel,' when present, being situated between the dentine and cement. The dentine, which is divided by Owen into hard or true dentine, vaso-dentine, and osteo-dentine, consists of an organised animal basis, disposed in the form of extremely minute tubes and cells, and of earthy particles.
The tubes and cells contain, besides the calceous particles, a colourless fluid, which is probably transuded blood plasma, or liquor sanguinis, and contributes to the nutrition of the dentine. In hard or true dentine the dental tubes proceed from the hollow of the tooth known as the pulp cavity, in a slightly wavy course, nearly at right angles to the outer surface. 'The hard substance of the tooth is thus arranged in hollow columns, perpendicular to the plane of pressure, and a certain elasticity results from these curves; they are upright where the grinding surface of the crown receives the appulse of the opposing tooth, and are horizontal where they have to resist the pressure of contiguous teeth.'
The tubuli also receive the plasma transuded from the remains of the vascular pulp, which circulates by anastomosing branches of the tubuli through the dentine, maintaining a sufficient though languid vitality of the system. The delicate nerve-branches on the pulp's surface convey sensations of impressions affecting the dentine—sensations of which every one has experienced the acuteness when decay has affected the dentine, or when mechanical or chemical stimuli have "set the teeth on edge." When a part of the primitive vascular pulp from which the dentine is developed remains permanently uncalcified, red blood is carried by 'vascular canals' into the substance of the tissue. Such dentine is called vaso-dentine, and is often combined with true dentine in the same tooth, as, for example, in the large incisors of certain rodents, the tusks of the elephant, and the molars of the extinct megatherium. When the cellular basis is arranged in concentric layers around the vascular canals, and contains 'radiated cells,' like those of bone, this is termed osteo-dentine, and resembles true bone very closely. The cement always corresponds in texture with the osseous tissue of the same animal, and wherever it occurs in sufficient thickness, as on the teeth of the horse or ox, it is traversed like bone by vascular canals. Moreover, when the osseous tissue contains minute radiated cells, precisely similar cells are likewise present in the canal, and constitute its most marked characteristic. The relative densities of dentine and cement vary according to the amount of earthy matter. In the complex grinders of the elephant and some other animals the cement, which forms nearly half the mass of the tooth, wears down sooner than the dentine. The enamel is the hardest of all the animal tissues, and contains no less than 96.4 per cent. of earthy matter (mainly phosphate of lime), while dentine contains only 72 per cent., and cement and ordinary bone only 69 per cent. of earthy matter. The earthy matter is contained in comparatively wide canals, composed of animal membrane of extreme tenacity.
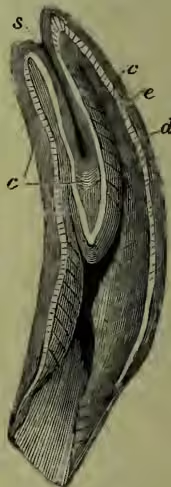
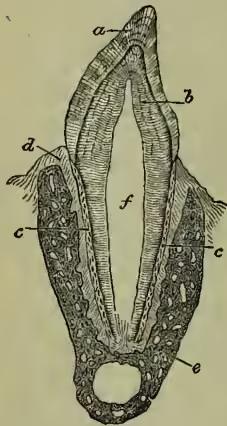
In a few fishes the teeth consist of a single tissue—a very hard kind of non-vascular dentine. Teeth consisting of dentine and vaso-dentine are very common in fishes. Dentine and cement constitute the grinding teeth of the dugong. In the teeth of the sloth the hard dentine is reduced to a thin layer. 'The human teeth and those of the carnivorous mammals appear at first sight to be composed of dentine and enamel only; but their crowns are originally, and their fangs are always covered by a thin coat of cement. There is also commonly a small central tract of osteo-dentine in old teeth. The teeth called compound or complex in mammalia differ as regards their composition from the preceding only by the different proportion and disposition of the constituent tissues. Fig. 2 is a longitudinal section of the incisor of a horse; d is the dentine, e the enamel, and c the cement, a layer of which is reflected into the deep central depression of the crown; s indicates the coloured mass of tartar and particles of food which fills up the cavity, forming the "mark" of the horse-dealer.' Far more complex forms of teeth than this may be produced by peculiar arrangements, chiefly inflections, of the tissues (see LABYRINTHODONTS). Another kind of complication is produced by an aggregation of many simple teeth into a single mass, as in some fishes and a few mammals. The teeth of the Aard-vark (q.v.) are of this kind, each tooth being composed of a congeries of long and slender prismatic denticles of dentine, which are cemented together. In the elephant the compound molars belong to this class, the denticles being in the form of plates vertical to the grinding surface, and transverse to the long diameter of the tooth.
The teeth of fishes, in regard to their number, form, substance, structure, situation, or mode of attachment, offer a greater and more striking series of varieties than do those of any other class of animals. In all fishes the teeth are shed and renewed, not once only, as in mammals, but frequently during the whole course of their lives. Tortoises and turtles, toads, and certain extinct Saurians are toothless. Frogs have teeth in the upper, but not in the lower jaw. Newts and salamanders have teeth in both jaws and upon the palate; and teeth are found on the palate as well as on the jaws of most serpents. In reptiles, as a general rule, the base of the tooth is anchylosed to the bone which supports it. The completion of a tooth is soon followed by preparation for its removal and succession, the faculty of developing new tooth-germs being apparently unlimited in this class. The extinct Odontornithes (q.v.) are the only birds with teeth. Of mammals there are a few genera and species devoid of teeth. The true ant-eaters, the pangolins, and the echidna are strictly toothless. The ornithorhynchus has horny teeth, and the whales have transitory teeth, succeeded in the upper jaw by whalebone. The Narwhal (q.v.) has a peculiar development. The elephant has never more than one entire molar, or parts of two, in use on each side of the upper and lower jaws; to which are added two tusks, which are modified incisors, more or less developed, in the upper jaw. The boar's tusks are large and powerful canines. Some rodents have two grinders on each side of both jaws, which, added to the four cutting-teeth in front, make twelve in all; but the common number of teeth in this order is twenty, although hares and rabbits have twenty-eight each. The number of teeth, thirty-two, which characterises man, the apes of the old world, and the true ruminants, is the average one of the mammals. The dentition is often summarised as to the number and position of incisors, canines, molars, and premolars, thus: the dental formula of the typical mammal is inc. , can. , pm. , m. ; or more briefly . The absent teeth may be denoted by or by a blank. The dentition is indicated in the articles on the several animals where it is of interest (especially at HORSE), and in the articles on the great groups of animals (see, for example, CARNIVORA). Dolphins may have 200 teeth. (Compare the number of teeth on the tongue of the common garden snail; 135 rows of 105 teeth each—14,175 in all.) It is only in the mammals that we have a well-marked division of the teeth into the four kinds of incisors, canines, premolars, and molars, each of which claims a brief description.
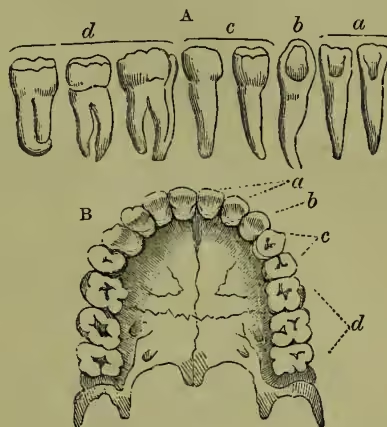
The incisors, or cutting-teeth, are situated in front, and possess a single conical root or fang, and a vertical crown bevelled behind, so as to terminate in a sharp cutting edge. These teeth are specially fitted, as their name implies, for cutting the food. In man there are two of these incisors in each side of each jaw (in the pre-maxilla). The permanent incisors, molars, and premolars are preceded by a set of deciduous or milk teeth, which are lost before maturity, and replaced by the permanent ones. In herbivorous animals they crop the herbage; in rodents (the rabbit, hare, rat, beaver, &c.) these teeth are very much developed, and differ from any other teeth occurring in mammals in this respect, that their growth continues throughout life; and if their length does not constantly increase, it is because their free extremity or edge is worn down by trituration as fast as they grow at the base from their roots.
The canines (so called from their prominence in the dog) come next to the incisors. Their crown is rather conical than wedge-shaped, and their fang sinks more deeply into the jaw than in the case of the incisors. In all carnivorous animals they are largely developed, being obviously formed for tearing the flesh of their prey. In man there is one canine tooth in each half-jaw; and there is never more than this number in any of the lower animals.
The premolars (known also as bicuspid and false molars) come next in order to the canines; they are smaller than the latter, and their crown presents two pyramidal eminences. In man there are two premolars in each half-jaw. Their function more nearly approaches to that of the true molars behind them, than to that of the canines.
The true molars (or multicuspid) are placed most posteriorly. They are remarkable for their comparatively great size, the square form of the upper surface, on which are from three to five elevations or cusps, and for their short root, which is divided into from two to five branches, each of which is perforated at its extremity. They appear first in the permanent set. In man there are three molars in each half-jaw, the posterior one being termed the wisdom-tooth, from its being cut the latest; they are especially employed for grinding the food, under the action of the muscles of the lower jaw.
The teeth are so admirably adapted for the special purposes which they are called upon to fulfil that it is generally easy, from a careful examination of them, to say to what class of animals they belong, and to draw various conclusions regarding the habits and structure of the class generally. Thus, in carnivorous animals the molars are not grinding-teeth, but present sharp cutting edges, and those of the upper and lower jaw overlap each other, resembling a pair of scissors in their action. In insectivorous animals the molars have a tuberculated surface, with conical points and depressions, so arranged as to lock into each other. In frugivorous animals, living on soft fruits, these teeth are provided with rounded tubercles, while in herbivorous animals they have a broad, rough surface, resembling a millstone.
There is also a close connection between the articulation or joint of the lower jaw and the nature of the food used by the animal. Thus, in purely carnivorous animals, in which the teeth simply tear and cut the food, no grinding motion is required, and the jaw is capable only of a simple hinge-motion in the vertical plane; while in herbivorous animals the joint is so constructed as to allow of extensive sliding and lateral motion of the lower molar teeth upon the upper. In man both the form of this articulation and the general character of the teeth point to an intermediate position in relation to food, and form a physiological argument for the mixed diet which general custom has decided to be most natural to our species.
See the articles CARNIVORA, DOG, RODENTIA, SKULL, for illustrations of teeth in situ; and besides general works on anatomy, human and comparative, Owen's Odontography (1845) and other works, and Flower's Osteology of the Mammalia (1886).
DISEASES OF THE TEETH.—Decay (Caries) is by far the most common of the diseases which affect the teeth, and consists in a gradual and progressive disintegration of the tooth-substance. Among the chief predisposing causes are hereditary defects of quality; imperfect calcification; pits and grooves in the enamel; overcrowding of the teeth; facilitating the retention of particles of food between them, constitutional disorders; chiefly those affecting the digestive organs; and debilitating causes generally—e.g. over-exertion of nervous and mental energies. The exciting cause of caries has recently been proved by Professor Miller of Berlin to be due to the action of micro-organisms. According to him, 'the first stage of dental caries consists in the decalcification of the tissues of the teeth by acids which are for the greater part generated in the mouth by fermentation,' the agents concerned in the process being micro-organisms and the acid they produce—lactic acid.
Decay is rarely met with on smooth surfaces exposed to the friction of food and the direct washings of the saliva. It usually begins in some pit or groove in the enamel or between the teeth, such points forming a lodgment for the development of the organisms. Once the enamel has been penetrated the decay proceeds more rapidly, spreading laterally beneath the as yet healthy enamel and towards the pulp. The more dense the structure of the tooth the more directly does the decay penetrate in the direction of the pulp, although its progress is not so rapid and its tendency to spread is less. Caries is most common in early life, by far the greater number of cavities making their appearance between the ages of six and eighteen. Its colour varies from pale brown to black, and generally the lighter the colour the more rapid is the decay. Pain may be felt soon after the enamel has been penetrated, or may be delayed until the nerve (pulp) has become almost or quite exposed; yet, strangely enough, it is sometimes altogether absent, particularly in very hard teeth. When the pulp has become nearly encroached upon, the patient's sensations will warn him against taking hot or cold, sweet or acid fluids. Ultimately the pulp becomes exposed, when the pain increases and may become very violent, especially if the nerve be pressed upon by food forced into the cavity by mastication. Should this take place the pulp becomes acutely inflamed and soon dies, when the pain may either cease or go on till an alveolar abscess is formed. The treatment of caries can only be undertaken by the dentist, and varies with the extent and character of the disease. See DENTISTRY.
Periostitis and Alveolar Abscess.—Periostitis is an inflammation of the membrane (periosteum) which covers the roots of the teeth and lines their sockets. It may be either general or local. When general the majority or all of the teeth are commonly involved. Periostitis of this type is usually due to constitutional causes (such as rheumatism), or the effects of some such agent in the system as mercury, or the presence of accumulated tartar about the necks of the teeth. When the disease is local—confined to one or two teeth—it may result from a blow or some such injury, or it may proceed from an inflamed pulp; but by far the most common cause is the presence of a dead nerve, the poisonous products of which are liable at any time to cause violent inflammation at the end of the root. Yet it is not uncommon to find that teeth whose pulp dies and whose substance gradually breaks down and decays away do not give rise to any trouble. When acute periostitis has fairly set in, it and its usual accompaniment, alveolar abscess, are perhaps the most painful affections to which the teeth are subject. The symptoms vary in intensity, though the characters remain the same. A dull aching pain is felt, and is relieved at first by pressure upon the affected tooth; as the inflammation increases in severity the tooth rises slightly in its socket, and becomes exquisitely painful when bitten upon; the gum around it becomes congested, and the throbbing pain is almost continuous.
Alveolar Abscess may be defined as a suppuration around the root or roots of a tooth. It is of two varieties, acute and chronic. Its causes are those of periostitis, which precedes it, the continuous and throbbing nature of the pain indicating the formation of matter (pus) within the surrounding bone. The face, with the glands about the neck, swell, and the glands exhibit tenderness on touch. The pent-up pus forces its way through the bone to reach the surface of the gum at the point of least resistance, which is most often opposite the end of the root or roots (this is popularly known as a 'gum-boil'). It occasionally finds its way along a canal by the side of the root, and discharges at the edge of the gum. Sometimes the discharge burrows downwards to find an exit on the face. This is almost peculiar to the lower teeth, and calls for removal of the tooth affected. With the escape of pus by 'gum-boil' there is a marked abatement in the intensity of the pain, which generally disappears in a few hours and the swelling in a few days. If left to itself, however, the abscess soon assumes the chronic form, the tooth becoming almost if not quite comfortable. This condition may continue for an indefinite period, but there may also be a recurrence of the symptoms in a milder form. Not unfrequently chronic abscesses occur without giving rise to any pain, the only evidence of their existence often being a small fistulous opening on the surface of the gum, from which from time to time pus discharges. Even this last may be wanting. If the abscess resist all treatment, the disease can be cut short by the extraction of the tooth, although many cases can be successfully treated and the tooth rendered permanently useful.
Exostosis is characterised by an increase in the thickness of the cementum, the external of the two hard tissues forming the roots of the teeth. Its forms vary from a small nodule or patch to a quantity sufficient to invest the entire root or roots of the same or adjoining teeth. It is most often caused by slight but continued irritation of the periosteum by caries, or by rapid wearing of the masticating surfaces. Occurring as it sometimes does in teeth otherwise sound, its diagnosis is difficult; its presence may not be suspected till an attempt is made to extract the tooth, which, owing to the enlargement of the fangs, cannot even when loosened be removed without great difficulty. Exostosis may often cause neuralgic pains about the jaws.
Impaction and difficult Eruption of the Wisdom and other Teeth.—It is not uncommon to find certain of the temporary teeth firmly set in the adult jaw, and occupying the place of the permanent ones. In such cases the permanent tooth is usually present in the body of the jaw, but it has been retarded in eruption by being too deeply imbedded in the bone. Impaction may also be due to an abnormal direction of growth. Such teeth may appear late in life after all the others are lost, and the bone overlying them has been absorbed and so exposed them. When these cases do occur they are responsible for the popular but incorrect idea of a third set of teeth. An impacted tooth seldom gives rise to any trouble, unless it be an upper or lower wisdom, particularly the latter. The cutting of these teeth is sometimes accompanied by distressing symptoms which may be protracted for months or years, unless they are removed by extraction of the tooth. This condition is usually due to imperfect development of the jaw. The tooth usually takes its natural vertical direction, but, being wedged in between the tooth in front and the ascending portion of the jaw behind, only a small portion of the crown is visible. The overlying gum is apt to be bruised by the occlusion of the opposing tooth in the upper jaw; inflammation is thereupon set up, and being maintained by biting may extend to the surrounding parts. Swallowing becomes painful and the motion of the jaws restricted. When it is evident that there is insufficient accommodation in the jaw for the erupting tooth it should be removed.
Inflammation of the Gums, although not a disease of the teeth proper, is one of the most common causes of their premature loss. It may arise from constitutional causes—chronic dyspepsia, rheumatism or gout—or from the administration of such drugs as mercury or iodide of potassium. Most often, however, it results from the presence of tartar about the necks of the teeth, and lack of thorough cleansing. When due to constitutional causes, their appropriate remedies are called for; but when due to the presence of tartar, this deposit should be carefully removed. See DENTISTRY (Scaling).
Absorption of the Alveoli.—The gradual wasting of the bone which surrounds and supports the roots of the teeth, accompanied by a simultaneous recession of the gums, is one of the changes which mark the approach of old age. This wasting may, however, occur in middle life without any visible cause, although the majority of such cases are due to chronic inflammation of the gums, with or without the deposition of tartar. Heredity, or the use of too hard a tooth-brush, may likewise be accountable. The teeth most affected are the front ones; but the reverse of this is not unusual. The gums, especially in front, gradually recede and lay bare the roots; the teeth now become loosened and finally drop out. The treatment consists in the removal of any obvious source of irritation; but when the disease is due to heredity nothing can be done to arrest its course.
Abrasion of the Teeth is a gradual loss of their substance from causes which are purely mechanical. The more common cause is a faulty occlusion of the jaws, but it is also produced by the improper use of the tooth-brush. When the result of mal-occlusion, it shows itself upon the grinding surfaces of the back teeth and the cutting edges of the incisors, which may become rapidly worn down almost to the gum, the rate of progress being frequently hastened by the common habit of grinding the teeth together. When caused by improper brushing it is seen on the front surfaces.
Erosion of the Teeth, on the other hand, though closely resembling the second form of abrasion, is understood to be due to the secretion of a corrosive acid by the labial glands. It is first seen near the gums as a small concave depression with a smooth polished and often very sensitive surface continuous with the front of the tooth. As it progresses, the pulp recedes, throwing out successive layers of protective dentine until it becomes entirely calcified. The disease can generally be arrested by filling, preferably with gold or porcelain inlays.
Diseases of the Antrum, while springing from other sources, are often caused by diseased teeth. The cavity in the bone of the upper jaw, known as the Antrum of Highmore, communicates by a small opening with the nose, and is sometimes the seat of inflammation set up by the presence of an abscess in connection with one of the back teeth, the roots of which project into it. The most common symptom of such a condition is an offensive discharge from the nostril of the affected side, increased in quantity when the patient lies down. The treatment is very tedious, much depending upon the age and general health of the patient; it consists in the removal of any diseased teeth from the affected side. This extraction may be followed by a discharge of pus; if not, an opening into the antrum should be made through the socket of one of the roots, and the cavity drained, suitable stimulating and disinfecting lotions being injected by means of a syringe till a healthy condition is established. Among the less common forms of disease which attack the teeth and gums are necrosis, dentigerous cysts, odontomes, epuloid and polypoid and other tumours of the jaws, and diseases of the tooth-pulp itself. These, however, are so comparatively rare as to be of no interest to the general reader.
Toothache is not so much a disease as a symptom. Its chief causes are mentioned under Caries and Alveolar Abscess. The pain, which varies greatly in degree, character, and duration, depends largely upon its cause, and the health of the patient at the time of the attack. Only a transient uneasiness may in some instances be felt, and, as often, in others almost insupportable agony. If neuralgic in character it most frequently occurs in paroxysms at more or less regular intervals. When toothache is due to caries with or without simple exposure of the pulp, the attack is brought on by taking hot or cold, sweet or acid fluids, and is seldom of long duration. To afford relief in such cases as these, gently wash out the cavity with a solution of carbonate of soda; then, drying it carefully with a piece of cotton-wool, take a very small pellet of wool dipped in encalyptus oil and place it in the bottom of the cavity; over this place a piece of cotton-wool large enough to fill the cavity and saturated with the following solution: 1 drachm of mastic in ounce of Eau de Cologne. This should be changed daily. When the pain is caused by the forming of an alveolar abscess the tooth will be found insensitive to change of temperature but very susceptible to pressure. The patient now becomes feverish, and the pain, which is at first of a dull heavy character, becomes more intense, throbbing, and continuous, till pus has been formed and discharged through the gum. Provided the tooth is likely to prove useful and the patient cannot consult a dentist, the gum should be carefully painted with tincture of iodine, or the old-fashioned plan of placing a roasted fig over the root may be resorted to; at the same time it is well to give an aperient such as Epsom salts, followed by a full dose of quinine—6 to 8 grains for an adult. Great relief follows this treatment, which is, of course, only temporary. If an abscess shows signs of pointing upon the gums it may with advantage be lanced. Poultices must never be applied to the face, for heat tends to draw the pus outwards. Abscesses in connection with the lower wisdoms often assume a very serious character unless cut short by extraction of the tooth.
Hygienic Care of the Teeth.—Many of the diseases of the teeth and gums might be prevented or greatly retarded by proper attention to the cleansing of these organs. The implements best fitted for this purpose comprise the quill toothpick, waxed silk thread and brushes, with suitable powders. The toothpick ought to be used after every meal, but it should be supplemented by the use, between the teeth, of floss silk, which will remove deposits accumulating where contiguous teeth touch. The brush is used to remove all deposits solid and mucous, and it gives the teeth a bright and polished appearance; its mechanical friction too stimulates the gums to more healthful action. An excellent tooth-powder is composed of precipitated chalk, 2 ounces; light magnesia, 2 ounces; oil of cinnamon, 8 drops; thymol crystals, 4 grains; otto of roses, 10 drops. The teeth should be brushed twice daily, in the morning and in the evening. The manner of using the brush is more important than many people suppose. The general method is to brush horizontally, but a moment's reflection will show that this leaves untouched the very situations most in need of cleansing. The brush, used properly, should be pressed against the teeth and the handle rotated so as to make the bristles sweep vertically between and over them; this, coupled with an up-and-down motion, will thoroughly cleanse the interspaces; the inner surfaces of the back teeth are best cleaned in a like manner, while the corresponding parts of the upper and lower incisors are effectually reached by a vertical drawing movement. The brush should be of medium texture, and the bristles of unequal length, and not too closely placed. A hard-and-fast rule cannot, of course, be laid down for everyone to follow, but in the majority of cases it is advisable to use the powder in the morning and a mouth-wash with the brush in the evening. For the latter purpose the following is good (especially where a tendency to inflammation exists)—tannic acid, 4 grains; rose water, 1 ounce; tincture of pyrethrum, drachm; oil of cinnamon, 10 drops. Over-brushing must be guarded against as carefully as under-brushing lest the gums and the necks of the teeth be injured. During an illness these precautions are doubly necessary as the corrosive effects of many medicines are then added to the civil results of a weakened vitality. The use of a glass tube in taking medicines that contain mineral acids and iron is usually supposed to be a sufficient precaution against the action of such drugs upon the teeth, but this is quite erroneous; the only sure preventative being a weak solution of ordinary baking soda, with which the mouth should be rinsed after every dose. The choice of a tooth-powder should be left to the dentist, for many dentifrices which, no doubt, whiten the teeth do so by the action of some agent which is as deadly to the tooth-substance as to the impurities it is meant to remove. Charcoal (so much used) is quite unsuitable because of its gritty nature. As far as the ordinary individual is concerned, the use of brush and toothpick is the limit up to which one can take care of one's own teeth, so that a thorough examination of the mouth once or twice a year by a trustworthy professional man is necessary to check the diseases of the teeth before they have gone so far as to be irreparable. Especially should this be attended to in children. It is almost impossible to overrate the importance of following, at least in the main if not in detail, the hints given above, for when we consider that the teeth are placed at the very gateway of life, it is not surprising that their neglect should be answerable for many of the disorders of the system. And surely precaution is better than cure.
For a more detailed description of the diseases of the teeth, see the works of Litch, Tomes, and Salter.