Tubercle is the characteristic product of a specific micro-organism, the Bacillus tuberculosis. It is a new formation, belonging to the group of Granulomata or granulative growths, which, in virtue of their recognised infectiveness, have been classed as Infective Granulomata. Tuberculosis (see CONSUMPTION, SCROFULA) is a specific infective disease, induced by the invasion of the Bacillus tuberculosis, and characterised by the presence of tubercle or other tuberculous formation. Tuberculosis is local or general, according to the distribution of the infection.
Prior to 1882 it would have been impossible to define tubercle in those words. Tubercle is, nevertheless, a term of great antiquity. Its connotation has varied considerably, and this has been the source of much confusion. By older writers, and up till the beginning of the 19th century, tubercle was used to signify a nodule, or small indurated mass. Such indurated masses (scirrhosities) had been recognised in the lungs and elsewhere. But in the description of these, tubercle had a morphological rather than an etiological significance; its application was not restricted to the product of a particular pathological process. With the development of anatomical study in the 17th and 18th centuries, these 'tubercles' of the lung received much attention; but they were misunderstood and interpreted incorrectly. Some observers spoke of them as altered glands. Sydenham speaks indifferently of 'glandules' and 'tubercles' arising in the lungs. Cullen recognised in tubercles one of the most frequent causes of pulmonary phthisis, but he did not attempt further definition than 'small tumours which have the appearance of indurated glands.' In the 18th century the occurrence of widely disseminated and more or less uniformly distributed tubercle—miliary tubercle of later times—was recognised. The classic comparison between such tubercle and the millet seed had been established—a comparison which has survived to our times and is in use in the schools by some who have never identified the millet seed.
Early in the 19th century the anatomical conception of tubercle was merged in the etiological through the work of the French physicians Bayle and Laennec (see CONSUMPTION), who expounded the view that 'consumption was essentially due to the presence in the lung of little granular masses of varying size and character.' This was the first suggestion of tuberculosis as a synonym for consumption or phthisis. The tubercular degeneration Bayle (1810) held was 'a chronic, specific affection, quite independent of any glandular or lymphatic inflammation.' This view was advocated strongly by Laennec (1834), who recognised four forms of tubercle—viz. (1) miliary, (2) crude, (3) granular, (4) encysted; and later by the French clinician, Louis. Their united teaching led to the earliest crystallisation of the doctrine of tuberculosis, and proved the basis of much after-work.
The weight of Virchow's powerful argument (Die krankhaften Geschwülste, 1865) was directed against the view of a common specific element in Laennec's four groups. He concluded rather that the 'crude,' or yellow tubercle, was a product of retrograde cellular metamorphosis, and he limited the term tubercle to the first of Laennec's varieties. He emphasised the appearance of caseation or necrosis of the tissue elements, which occurs in tubercular (and other) foci, and thought that if a sufficiently careful examination were made, a precedent condition of caseation would be discovered, in nearly every instance, in relation to the eruption of tubercle. From the clinical side this view received support from Niemeyer (1866), who held that the order of events in most cases of consumption was the occurrence of a 'catarrhal pneumonia,' which might resolve naturally, or might be followed by the process of caseation or cheesy degeneration. A 'caseous catarrhal pneumonia' was followed by breaking down of the lung tissues and the establishment of the condition of 'phthisis.' The eruption of tubercle proper was, according to Niemeyer, a secondary feature. Most cases of 'phthisis' were to be traced to the effects of 'neglected cold,' and Niemeyer believed that the assertion of Laennec and his followers, that such 'colds' had little influence, was fatal both to prophylaxis and treatment.
A new phase in the pathology of tubercle was inaugurated by the experimental researches of Villemín (1865), who, on introducing caseating material or the expectoration of phthisical patients subcutaneously into rabbits and other animals, found that they became tuberculous—i.e. that tubercles were discoverable in many of their viscera in periods varying from three to six weeks. This result followed the introduction of such material only. This led Villemín to the conclusion that tuberculosis was a specific inoculable disease, to be ranked along with other known infective processes. He believed that infection might result from inoculation, contagion, or the absorption of germs suspended in the air. Those views, though questioned at first, were fully confirmed by subsequent observers, some of the keenest critics (Cohnheim, Sanderson, Wilson Fox) being converted by a repetition of their own experiments. The following conclusions which were put in writing in 1866, as the result of ten years' observation and reflection by Dr William Budd of Clifton, form a most important landmark in the history of this question. In the light of more recent knowledge, they testify in an eminent degree to the prescience of their author. They are—(1) 'that tubercle is a true zymotic disease of specific nature in the same sense as typhoid fever, scarlet fever, typhus, syphilis, &c.; (2) that, like these diseases, tubercle never originates spontaneously, but is perpetuated solely by the law of continuous succession; (3) that the tuberculous matter itself is (or includes) the specific morbid matter of the disease, and constitutes the material by which phthisis is propagated from one person to another and disseminated through society; (4) that the deposits of this matter are, therefore, of the nature of an eruption, and bear the same relation to the disease phthisis as the 'yellow matter' of typhoid fever, for instance, bears to typhoid fever; (5) that, by the destruction of this matter on its issue from the body, by means of proper chemicals or otherwise—seconded by good sanitary conditions—there is reason to hope that we may eventually, and possibly at no very distant time, rid ourselves entirely of this fatal scourge.'
During the next fifteen years opinion gradually inclined more widely to the specific doctrine of tuberculosis. In 1880 Cohnheim declared that 'neither the nodular form, the histological structure, the occurrence of giant-cells, caseation, nor all these circumstances together are absolutely characteristic of tuberculosis. The only absolutely perfect and certain criterion is the capacity for infection.' At the end of 1881 Koch announced the discovery of the Bacillus tuberculosis. He proved that this organism was discoverable in all varieties of tuberculous disease; that a pure culture of the bacillus might be obtained artificially (see GERM THEORY); and that inoculation of animals with bacilli derived from such cultivation certainly led to a reproduction of the disease, with the characteristic development of further bacilli in the tissues. Koch was thus in a position to claim that the bacillus he had discovered was not only one, but the only, cause of tuberculosis, and that without the Bacillus tuberculosis there could be no tuberculosis. Most searching criticism and observation failed to invalidate his conclusions, and all subsequent experiment has attested the accuracy of his results. Koch's brilliant discovery has ended the fight over tubercle, and sanctioned the definition which prefaces the present article, that tubercle is a new growth, the characteristic product of the Bacillus tuberculosis.
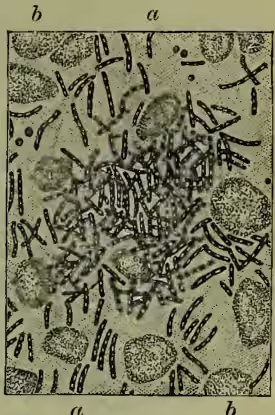
The tubercle bacillus is a delicate rod-like body (see BACTERIA) of varying length, averaging one-third the diameter of a red blood-corpuscle (circa inch), and approximately one-sixth as broad as it is long. With a powerful microscope, the individual rods present (fig. 1, a) a slightly curved form and frequently a beaded outline attributed to the presence of spores, but more probably the expression of vacuolation. The bacilli occur either singly or in groups. They may be discovered in one or several of the organs of the affected subject, in the blood, in the expectoration (fig. 1), in the urine, or other excretion. They have the special property of being stained in peculiarly 'fast' degree by certain of the aniline dyes. The bacillus may be cultivated artificially on sterilised blood-serum and other media. The organism is particular as to the nutrient soil, of slow growth, and requires a constant temperature of 86° to 105.8° F. Those facts would seem to indicate that a certain predisposition of tissues plays an important part in the determination of its development in the human subject.
Its distribution in the affected subject varies much. It may be either universally disseminated or localised. In the former case the distribution occurs presumably by way of the blood-stream; in the latter, by way of the lymphatic channels or by continuous growth over contiguous surfaces—e.g. over mucous or serous membranes. It may be carried from the original seat of infection to distant parts, where its arrest leads to the production of the characteristic new growth. General miliary tuberculosis may be induced in this way. The organism is also the cause of other conditions, where the eruption of tubercle proper is less observable or is even absent—e.g. glandular and some varieties of pulmonary and intestinal tuberculosis, in all of which, however, the infective agent is the same. Even when tuberculosis is general certain organs or tissues are selected for special deposit—e.g. the lung and serous surfaces (pleura, peritoneum, meninges). Various names are in use, according to the organ or structure which is affected, to differentiate the condition from that of simple or other specific inflammation of the given part. Thus, we speak of tuberculous meningitis, tuberculous peritonitis, pulmonary tuberculosis, renal tuberculosis, &c. But tubercle may be found in almost every part—e.g. lung, larynx, intestine, liver, spleen, kidney, bladder, testicle, brain, choroid coat of eye, bone, skin, blood-vessel, &c. When localised, the lung is the favourite seat. Most cases of general tuberculosis are traceable to an earlier local focus. Thus, general tuberculosis sometimes follows rude interference with localised disease, through the consequent absorption of the tubercle bacillus into the blood-stream. This general or miliary tuberculosis is an acute inflammatory condition with symptoms indicative of severe involvement of the system—e.g. rapid wasting and grave prostration. The course of the disease may resemble to a remarkable degree that of enteric (typhoid) fever, with which, indeed, it is sometimes confounded.
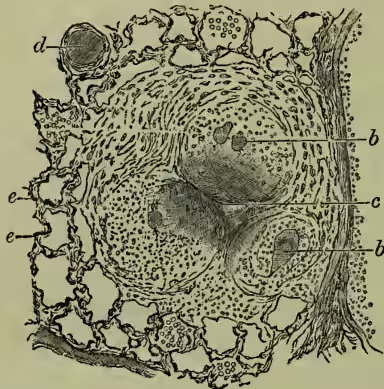
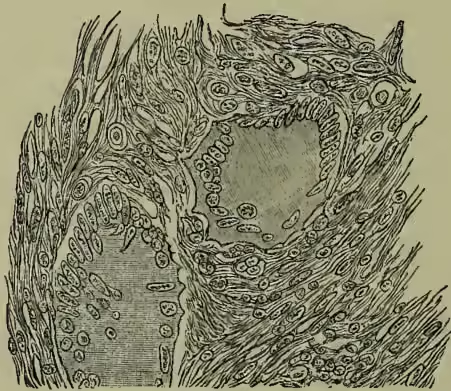
Anatomical Characters of Tubercle.—The typical tubercle is essentially a non-vascular nodule. It occurs usually in groups (fig. 2). The nodules bb, giant cells; c, centre of tubercle beginning to caseate; d, branch of pulmonary artery; e, alveolar framework of lung. (After Hamilton.) are seen easily by the unaided eye. They are of more or less round shape, and in size approximate a mustard seed. Their outline is well defined and, in the early stage, the colour is grayish. The surface presents a characteristic shimmer. Older nodules, which have undergone degeneration (see below), lose this appearance and assume a whitish-yellow colour. When examined microscopically the tubercle presents, in most instances, a special structure. But this is not constant. The centre is differentiated by the presence of one or more so-called 'giant-cells' (fig. 3). This is a large multinucleated cell, in which the nuclei are disposed in more or less radiating fashion round the periphery. The cell may, or may not, contain the tubercle bacillus. From the edge of the giant-cell delicate processes stretch outwards. These form a reticulum, in the meshes of which there occur large epithelium-like cells—so-called 'epithelioid' cells—and still more externally are found smaller rounded cells with one nucleus. But neither the giant-cell nor these other cells can be regarded as absolutely distinctive of tubercle. Atypical varieties of tubercle occur from which those are conspicuously absent, and whose structure appears to differ little from that of fibrous tissue.
Metamorphosis of Tubercle.—Tubercle is liable to certain metamorphoses—the so-called degenerations—commonest of which is the cheesy or caseous (fig. 2, c). The frequency of this led to much of the confusion which long existed on the subject. When caseating the tubercle assumes a more opaque and dull appearance, and its colour becomes whitish yellow. The advance of this process has been attributed to the absence of blood-vessels, and the toxic influence of the tubercle bacillus. It is a process of necrosis, or local death. On the other hand, the reticular elements may become more prominent and the nodule become fibrous.
Infectiveness.—Tuberculosis is contagious. The contagious element is the tubercle bacillus. Koch's early experiments with pure cultures, to which reference has been made, have been verified frequently. The tubercle bacillus has only to be introduced under the skin or into one of the closed cavities of the body to give rise to tuberculosis in the inoculated animal. The bacillus is found in enormous quantities in the sputum of consumptive patients. In some cases the expectoration contains an almost pure culture of the organism. It is to be found also in the juices and secretions of the body; thus it may occur in the milk of tubercular animals.
It may obtain access to the human subject. (1) By the respiratory passages. There is evidence for believing that this is most frequently due to the presence of dried particles of tubercular expectoration in the atmosphere. Hence the necessity of greater care than is usually exercised in the disposition of such sputum, and for the disinfection of rooms which have been long occupied by tubercular (consumptive) patients. The tubercle bacillus has been found clinging to the paper and curtains of such rooms, and from organisms thus collected pure cultures have been obtained. It is easy to induce tuberculosis in rabbits and other animals by exposing them in a confined space to the inhalation of a cloud of the dried particles of tubercular sputum. Similarly, the larynx seems to be affected secondarily by the contact of tubercular expectoration from the already affected chest.
(2) By the alimentary tract. Apparently the oesophagus and stomach are strongly resistant to the noxious influence. This is due probably to the frequent movement of the former and the presence of the gastric juice in the latter. The intestine, on the other hand, is readily infected. Thus the swallowing of tubercular matter may set up an intestinal process of this kind. Tuberculosis has been induced in animals whose food has been contaminated with such products. Domestic fowls are said to develop the affection from expectoration carelessly deposited in their vicinity. As has been seen, the milk from tuberculous cows may contain the organism—especially when the udder is affected—and such milk is certainly dangerous; hence the advisability of sterilising milk by exposing it to the influence of heat. Similarly, there is risk from the ingestion of the flesh of tubercular animals; hence the necessity for the thorough cooking of animal food. It has been proved experimentally that tubercular sputum, if boiled, is incapable of inducing the disease.
(3) By wounds. There can be no doubt that inoculation occurs in this way from time to time. But the frequency of such infection is not so great as might a priori have been expected. One meets cases, however, where, for example, tubercular sores of the hand have been so induced, and these have, in turn, been followed by involvement of the system generally. The disease known as Lupus is a peculiar, localised tuberculosis of the cutaneous tissues, which is probably traceable to superficial inoculation. Its limitation to the surface is charac- teristic. The tubercle bacillus has been found in the tissues affected by lupus, and general tuberculosis has occasionally followed surgical interference.
Heredity and Predisposition.—In many cases of tuberculosis there has existed admittedly a predisposition. It is difficult to define the nature and limits of such predisposition. But we may justly reduce the application of hereditary influence, as the phrase was formerly employed. We have to deal probably with the transmission of tissues which are somehow less resistant to the invasion of the special micro-organism. Parents weakened by various causes are likely to produce a progeny with such reduced power of resistance. It is recognised that tissues which resist strongly one variety of attack yield readily to another. Some families are specially liable to one or more of the infective processes, while resisting others. The same may be predicated of races of men and of animals. The influence of heredity may meanwhile be held to be manifested in the transmission to the offspring of tissues which possess a large susceptibility to, or at least a diminished power of resisting, the tubercle bacillus.
Products of Tuberculous Growth.—It has been long recognised that the growth of micro-organisms is associated with chemical alteration of the medium in which they develop. This explains the various fermentations, some of which are of much economic value. The artificial cultivation of special organisms has rendered knowledge of those processes and their products more exact. It has been recently proved that, in some instances, such products exert a prejudicial influence on the growing organism itself. When they are separated and mixed with cultivation media, the development of the particular organism has been found to be retarded or prevented. This is illustrated by the group of so-called Toxalbumins. In the year 1887 it was shown that tuberculous expectoration contained a substance or substances of eminently toxic character. Similar extracts were obtained from pure cultivations of the tubercle bacillus. Relatively small doses of these were found to produce serious or even lethal results in animals. More than one attempt was made to utilise those products in relation to the treatment of tuberculosis. In 1890 Koch announced that he had discovered a remedy of large efficacy in many tubercular conditions. In a later communication he detailed the nature of the agent—a forty to fifty per cent. glycerine solution of a pure cultivation of the tubercle bacillus. In this fluid there is present everything from the cultivation that is soluble in glycerine, including extractives, colouring matters, salts, &c. The apparently active part of the extract is insoluble in absolute alcohol, and can be thus separated in less impure form. Koch believes that the agent is a derivative from proteids, to which it is probably closely allied. But inasmuch as it withstands high temperatures and is easily dialysable, it seems likely that it does not belong to the group of Toxalbumins. To the fluid the name Tuberculin, or Tuberculinum Kochii, has been given. But from its character and mode of production it cannot be admitted that the fluid is of absolutely fixed constitution or strength. The introduction of a minimal amount of tuberculin into the subcutaneous tissues of the healthy subject is followed by no conspicuous phenomena. The dose requires to be considerable (0·25 c.c.) to induce pronounced symptoms, and these pass away comparatively rapidly. In the subject of tubercular disease, however, injection of a fractional amount of the fluid induces marked changes, both general and local. The general symptoms include rigor, fever, pain in the limbs, languor, vomiting, and cough; the local reaction, occurring at the seat of tubercular disease, and not at the point of injection, which is chosen indifferently, is best studied in superficial tuberculosis, especially lupus. In a few hours the parts become swollen and red; later, exudation appears on the surface, which dries and forms crusts. In typical cases the healing process goes on below these. A similar effect is produced, presumably, at tuberculous foci, which lie more deeply. Hence Koch was led to predicate both a therapeutic and a diagnostic value. Doubts have been expressed as to the extent of the former. It has been found that many cases of tuberculous disease have not improved much under its use. Attention has been drawn to the fact that there is a risk of a wider diffusion of the tuberculous disease through its use. On the other hand, it must be acknowledged that a number of cases treated with tuberculin have stood the test of time, and remained cured after several years. It is further certain that the risks which accompany its use in qualified hands have been disproportionately magnified. From the diagnostic point of view it has proved of great service, even if its value is lessened by the occasional occurrence of a reaction in subjects in whom there is no suspicion of tuberculosis. The attempts which have so far been made to purify tuberculin, including those by Koch, which resulted in a modified tuberculin (1897), have not been sufficiently successful to warrant more detailed reference.
A review of the experimental and clinical evidence which has been adduced leads to the conclusion that in the discovery and application of tuberculin a great advance has been made, and that solid ground has been touched in the diagnosis and treatment of tuberculous disease, through the elaboration of an agent related to the peccant organism, which has the power of detecting the presence and disturbing the progress of the disease. And there is reason to anticipate further advance on similar lines.
Tuberculosis in Animals.—Tuberculosis is of frequent occurrence among the lower animals. It is especially common in cows and, speaking generally, in stalled animals. 'Perlsucht,' regarding which there has been much discussion, has been proved identical with tuberculosis. The same bacillus is present in the bovine and human disease. There is reason to believe that the conditions of life, in the case of cows, render successful inoculation more likely, while there is the additional risk of contagion in the presence of an already affected animal. Domestic fowls suffer from the disease, as also caged rabbits and guinea-pigs. The latter animals take the disease readily by artificial inoculation. Probably fowl tuberculosis is due to another allied variety of bacillus. On the other hand, dogs, goats, and other animals of more active habits are less liable to infection. This fact has suggested the treatment of the condition in man by the transfusion of the serum of such animals. This has been attempted by several physicians with uncertain results. The rationale of the process is, however, doubtful (see GERM THEORY). When occurring in the lower animals the disease may be distributed generally, or restricted to special organs—for example, the lung or mamma. The milk of tuberculous animals, especially those whose udders are infected, has been found to contain the tubercle bacillus. The lesions produced by the bacillus are essentially the same as those which occur in the human subject.
Of the immense literature, reference may be made to Klebs, in vol. xx. of the Real-Encyclopädie der Gesamnten Heilkunde (2d ed.); Hamilton's Pathology, vol. i.; Fagge and Pye-Smith's Principles and Practice of Medicine. On special departments, see works bearing on this subject by Laennec (1834), Villemin (1868), Virchow (1863-65), Cohnheim (1879), Koch (1882-90), Bollinger (1883), Bang (1885), Woodhead, Heron (1890), and the writer of this article (1890).