Eye. In this article we shall consider: (1) The structure of the human eyeball, and of certain accessory parts or appendages which serve to protect that organ, and are essential to the due performance of its functions. (2) The most striking modifications which this organ presents in some of the lower animals. (3) The eye considered as an optical instrument. (4) The action of the retina. (5)
The movements of the eyeballs, and binocular vision.
(1) The globe of the eye is placed in the anterior part of the cavity of the orbit, in which it is held in position by its connection with the optic nerve posteriorly, by the muscles which surround it, and by the eyelids in front. It is further supported behind and on the sides by a quantity of loose fat, which fills up all the interstices of the orbit, and facilitates the various movements of which the eye is capable.
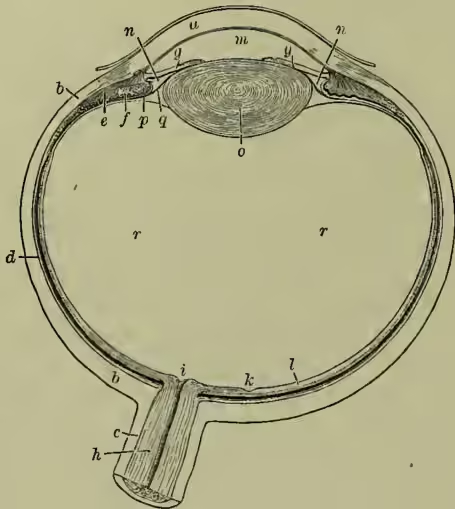
The form of the eyeball is nearly spherical; but on viewing the organ in profile we see that it is composed of segments of two spheres of different diameters. Of these, the anterior, formed by the transparent cornea, is more curved, and therefore more prominent. The horizontal transverse diameter is almost exactly an inch; the antero-posterior and vertical each about less. The radius of the posterior or sclerotic segment is about half, and that of the anterior segment about three-tenths of an inch.
When the eyes are in a state of repose, their antero-posterior axes are parallel; the optic nerves, on the other hand, diverge considerably from their commissure within the cavity of the skull to the point where they enter the globe; consequently their direction does not coincide with that of the eye. Each nerve enters the back of the globe at a distance of about one-eighth of an inch on the inner side of the antero-posterior axis of the eye.
The eyeball is composed of three concentric membranes, and of certain transparent structures, which are inclosed within them, and which, together with the cornea, transmit and refract the rays of light which enter the eye.
The outer (fibrous or protective) membrane consists of the sclerotic and cornea; the middle (vascular or nutrient) of the choroid and iris; the inner (nervous or perceptive) of the retina. The transparent contents are (from before backwards) aqueous humour, crystalline lens, and vitreous humour. We shall consider these structures in order.
The sclerotic (from skleros, 'hard'), or 'white of the eye,' is a strong, dense, fibrous structure, covering about five-sixths of the eyeball, and continuous, anteriorly, with the cornea. Posteriorly, it is perforated by the optic nerve, and it is there continuous with the sheath which that nerve derives from the dura mater, the fibrous investment of the brain and spinal cord. Near the entrance of the nerve, its thickness is about th of an inch; from this it diminishes to about th; but in front it again becomes thicker, from the tendinous insertions of the straight muscles which blend with it.
The cornea (so called from its horny appearance) is a transparent structure, continuous with the sclerotic, from which it differs more in appearance than in texture, and completing the fibrous tunic of the eye anteriorly. Its circumference is overlaid by the free edge of the sclerotic, as 'a watch-glass by the edge of the groove into which it is received.' Its thickness is from th to th of an inch. It is covered in front by a layer of conjunctival epithelium, which is exquisitely sensitive.
The cornea, in consequence of its greater convexity, projects beyond the line of the sclerotic; the degree of convexity, however, varies slightly in different persons, and at different periods of life. It is so strong as to be able to resist a force capable of rupturing the sclerotic. The fibrous coat, by its great strength and comparatively unyielding structure, maintains the inclosed parts in their proper form, and serves to protect them from external injuries.
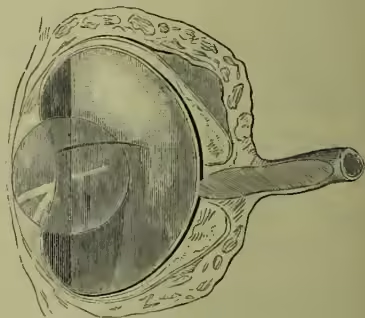
The choroid coat is a dark-coloured vascular membrane, which is brought into view on the removal of the sclerotic. Its outer surface, which is nearly black, is loosely connected with the sclerotic by connective tissue, in which are contained certain nerves and vessels—termed the ciliary nerves and vessels—some of which go forward to the iris. Its inner surface is smooth and dark-coloured. In front, it terminates in the ciliary processes (figs. 1 and 3), which consist of about sixty or seventy radiating folds or thickenings of the membrane, each of them terminated by a small free interior extremity, and lodged in a corresponding fold in the suspensory ligament of the lens. In other parts, it is covered by the hexagonal pigment-cells of the retina. The choroid is composed of minute ramifications of vessels— especially of veins, which, from their whirl-like arrangement, are termed vasa vorticosa—of connective tissue, and of large branching pigment-cells. Between the sclerotic and choroid at its anterior part lies a small but important structure, the ciliary muscle, which arises from the inner surface of the sclerotic near the cornea, and passes backwards to be inserted into the choroid opposite the ciliary processes.
The iris may be regarded as a process of the choroid, with which it is continuous, although there are differences of structure in the two membranes.
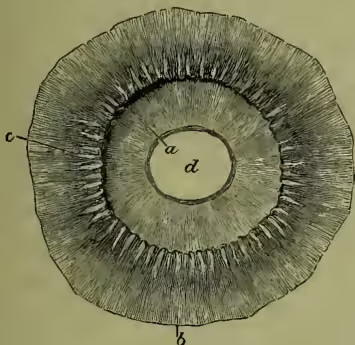
It is a thin flat membranous curtain, hanging nearly vertically in the aqueous humour in front of the lens, and perforated by the pupil for the transmission of light. Its anterior surface is variously coloured, and covered by fine irregularly-radiating projections; its posterior surface is smooth, and covered by a uniform layer of dark pigment, continuous with the pigment-cells of the retina. The posterior surface near the pupil is in contact with the anterior capsule of the lens. It divides the space between the cornea and the lens into an anterior (the larger) and a posterior (the smaller) chamber, these two chambers freely communicating through the pupil (see fig. 1). The outer and larger border is attached all round near the line of junction of the sclerotic and cornea, to the cornea, choroid, and ciliary muscle, while the inner edge forms the boundary of the pupil, which is nearly circular, and varies in size according to the action of the muscular fibres of the iris, so as to admit more or less light into the interior of the eyeball; its diameter varying, under these circumstances, from about d to th of an inch. It is muscular in its structure, one set of fibres being arranged circularly round the pupil, and, when necessary, effecting its contraction, while another set lie in a radiating direction from within outwards, and by their action dilate the pupil. These fibres are of the unstriped or involuntary variety. The nerves which are concerned in these movements will be presently noticed. The iris is richly supplied with blood-vessels; and pigment-cells like those of the choroid are scattered through its substance.
The varieties of colour in the eyes of different individuals, and of different kinds of animals, mainly depend upon the colour and amount of the pigment in these cells. In blue eyes, this pigment is scanty or absent, and the colour is due to the dark pigment of the posterior surface partly seen through the vascular membrane; in brown and black eyes, it is abundant, and is the cause of the colour. In albinos, this pigment is absent from iris, retina, and choroid, and hence their eyes have a pink appearance, which is due to the uncoagulated blood in the capillaries of the choroid and iris.
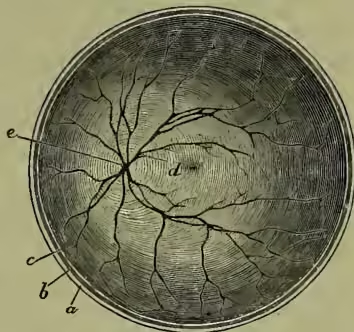
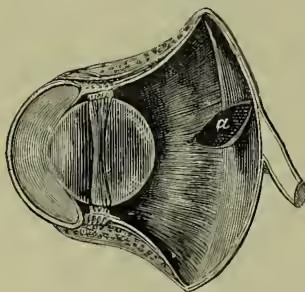
Within the choroid is the retina, which, although continuous with the optic nerve—of which it is usually regarded as a cuplike expansion—differs very materially from it in structure. Before noticing the elaborate composition of this part of the eye, which has only been revealed by microscopical investigation, we shall briefly mention those points regarding it which can be established by ordinary examination. It is a delicate semi-transparent sheet of nervous matter, lying immediately behind the vitreous humour, and extending from the optic nerve nearly as far as the lens. On examining the concave inner surface of the retina at the back of the eye (see fig. 4), we observe, directly in a line with the axis of the globe, a circular yellow spot (macula lutea), of about th of an inch in diameter, called, after its discoverer, the yellow spot of Sömmering, with a depression in its centre, the fovea centralis. About th of an inch internal to this is the entrance of the optic nerve, called the optic disc or papilla, from which the central artery and vein of the retina may be seen branching as they pass to their distribution.
The structure of the retina, as revealed by the microscope, is in the highest degree remarkable (see fig. 5). Although its greatest thickness (at the entrance of the optic nerve) is only about th of an inch, and as it extends anteriorly, it soon diminishes to th of an inch, the following layers from without inwards can be distinguished in most parts of it: (a) The pigmentary layer, consisting of a single layer of flat hexagonal cells, regularly arranged; its outer surface closely connected with the choroid, its inner in contact with the extremities of the rods and cones. Though its development shows that it really belongs to the retina, its mechanical connection with the choroid is firmer; and to this it adheres when the retina is stripped off. (b) The layer of rods and cones, frequently termed, from its discoverer, the membrane of Jacob; (c) outer granular layer; (d) outer molecular; (e) inner granular; (f) inner molecular; (g) layer of nerve-cells; (h) layer of nerve-fibres, in which the blood-vessels lie.
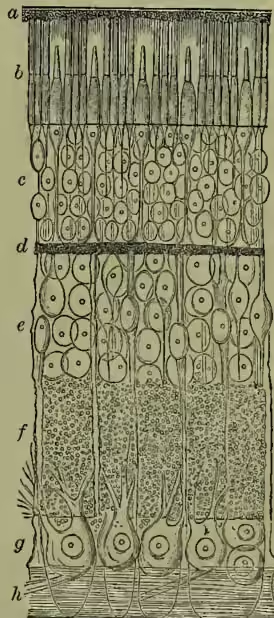
The layer of rods and cones, the portion of the eye which receives the impressions of light, deserves special attention. The rods are thinner but longer than the cones, and in most parts of the retina far more numerous. At the yellow spot, however, only cones are found. Each rod or cone consists of a thicker inner portion, connected with the outer granular layer, and ultimately with the optic nerve by a fine fibril; and an outer thinner part, directed towards and connected with the pigmentary layer. The perceptive elements are thus directed away from, not towards the light. 'In fact, we do not look outwards at the actual object, but we see the object as reflected from the base of our own eye.' Of the cones there are several, of the rods many millions in each human eye, and they are closely packed together over the whole extent of the retina.
It now remains for us to describe the transparent media which occupy the interior of the globe, and through which the rays of light must pass before they can reach the retina, and form on it the images of external objects. We shall consider them in the order in which the rays of light strike them.
Immediately behind the transparent cornea is the aqueous humour, which fills up the anterior and posterior chambers which lie between the cornea and the lens. As its name implies, it is very nearly pure water, with a mere trace of albumen and chloride of sodium. It is believed to be secreted by the choroid and to pass forward from it through minute lymphatic channels.
The crystalline lens lies opposite to and behind the pupil, in contact with the inner part of the iris, and its posterior surface is received into a corresponding depression on the forepart of the vitreous humour (see fig. 1). In form, it is a double-convex lens, with surfaces of unequal curvature, the posterior being the most convex. It is inclosed in a transparent capsule, of which the part covering the anterior surface is nearly four times thicker than that at the posterior aspect. The microscopic examination of the substance or body of the lens reveals a structure of wonderful beauty. Its whole mass is composed of extremely minute elongated ribbon-like structures, commonly called the fibres of the lens. These fibres are arranged side by side in lamellæ, of which many hundred exist in every lens, and which are so placed as to give to the anterior and posterior surfaces the appearance of a central star, with meridian lines. The lens gradually increases in density, and at the same time in refracting power, towards the centre; by this means, the refracting power is made greater than it would be even if the lens had throughout the same index of refraction as the nucleus. (According to the latest measurements, the index of refraction of the outer layer is 1.393; of the nucleus, 1.431; the total refractive power corresponds to that of a homogeneous body of the same size and shape with index 1.448.) This arrangement besides corrects to a certain extent the spherical aberration of the eye. According to Berzelius, the lens contains 58 per cent. of water, 36 of albumen, with minute quantities of salts, membrane, &c. In consequence of the albumen, it becomes hard and opaque on boiling, as we familiarly see in the case of the eyes of boiled fish. In the adult, its diameter transversely is about d, and its thickness antero-posteriorly about d of an inch; and it weighs three or four grains. The lens is held in position by the suspensory ligament of the lens and zonule of Zinn, a fine transparent fibrous structure, attached outwardly to the choroid between the ciliary processes, and passing inwards to blend with the anterior and posterior capsule of the lens near its margin (see fig. 1).
The vitreous humour lies in the concavity of the retina, and occupies about four-fifths of the eye posteriorly. Its form is shown in fig. 1. It is inclosed, except in front, in the hyaloid membrane, which blends anteriorly with the zonule of Zinn; and its anterior surface is in contact with the posterior capsule of the lens. It is quite transparent, and of a soft gelatinous consistence. Its outer part at least is laminated, like the coats of an onion. But the exact arrangement of the framework which gives it its consistence has not been determined. Between the anterior border of the retina and the border of the lens, we have a series of radiating folds or plaitings termed the ciliary processes of the vitreous body, into which the ciliary processes of the choroid dovetail. The vitreous humour contains, according to Berzelius, 98.4 per cent. of water with a trace of albumen and salts, and hence, as might be expected, its refractive index is almost identical with that of water.
The appendages of the eye now claim our notice. The most important of these appendages are the muscles within the orbit, the eyelids, the lachrymal apparatus, and the conjunctiva, to which (although less important) we may add the eyebrows.
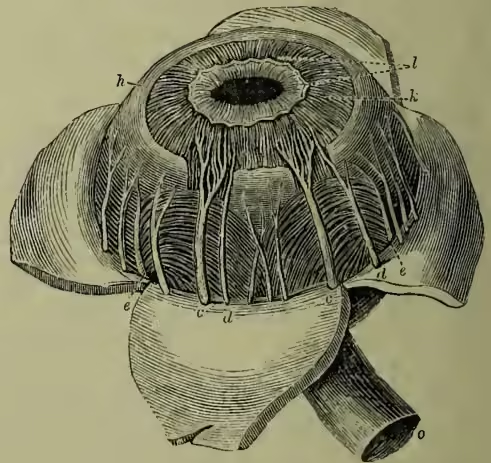
The muscles by which the eye is moved are four straight (or recti) muscles, and two oblique (the superior and inferior). The former arise from the margin of the optic foramen at the apex of the orbit, and are inserted into the sclerotic near the cornea, above, below, and on either side. The superior oblique arises with the straight muscles; but after running to the upper edge of the orbit, has its
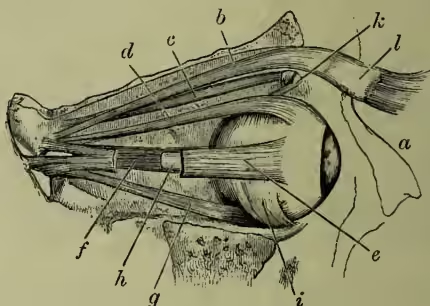
The external rectus muscle divided to show the optic nerve, which has also been cut to show the internal rectus muscle. a, nasal bone; b, levator palpebræ superioris; c, superior oblique; d, superior rectus; e, external rectus; f, internal rectus; g, inferior rectus; h, optic nerve; i, inferior oblique; k, pulley; l, tarsal cartilage. direction changed by a pulley, and proceeds backwards, outwards, and downwards (see fig. 6). The inferior oblique arises from the lower part of the orbit, and passes backwards, outwards, and upwards. The action of the straight muscles is sufficiently obvious from their direction: when acting collectively, they fix and retract the eye; and when acting singly, they turn it towards their respective sides. The oblique muscles antagonise the recti, and draw the eye forwards; the superior, acting above, directs the front of the eye downwards and outwards, and the inferior upwards and inwards. By the duly associated action of these muscles, the eye is enabled to move (within definite limits) in every direction.
The cyclids are two thin movable folds placed in front of the eye, to shield it from too strong light, and to protect its anterior surface. They are composed of (1) skin, with a layer of muscle (part of the orbicularis, see below) closely adherent to it; (2) of a thin plate of fibro-cartilage, termed the tarsal cartilage, the inner surface of which is grooved by thirty or forty parallel vertical lines, in which the Meibomian glands are imbedded; and (3) of a layer of mucous membrane (conjunctiva), continuous, as we shall presently see, with that which lines the nostrils, and joining the skin at the margin of the lids, in which the eyelashes (cilia) are arranged in two or more rows. The upper lid is much the larger; and to the posterior border of its cartilage a special muscle is attached, termed the levator palpebræ superioris, whose object is to elevate the lid, and thus open the eye; while there is another muscle, the orbicularis palpebrarum, which surrounds the orbit and eyelids, and by its contraction closes the eye. The Meibomian glands secrete a sebaceous matter, which facilitates the free motion of the lids, and prevents their adhesion. The eyelashes intercept the entrance of foreign particles directed against the eye, and assist in shading that organ from an excess of light.
The lachrymal apparatus consists of the lachrymal gland, by which the tears are secreted; two canals, into which the tears are received near the inner angle of the eye; the sac, into which these canals open; and the duct, through which the tears
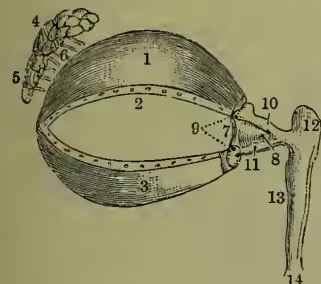
The Appendages of the Eye: 1, the cartilage of the upper eyelid; 2, its lower border, showing the openings of the Meibomian glands; 3, the cartilage of the lower eyelid, also showing on its border the openings of the Meibomian glands; 4, 5, the lachrymal gland; 6, its ducts; 7, the pleia semilunaris; 8, the caruncula lachrymalis; 9, the puncta lachrymalia, opening into the lachrymal canals; 10, 11, the superior and inferior lachrymal canals; 12, the lachrymal sac; 13, the nasal duct, terminating at 14 in the lower meatus of the nose. pass from the sac into the nose. The gland is an oblong body, about the size of a small almond, lying in a depression in the upper and outer part of the orbit. The fluid secreted by it reaches the surface of the eye by twelve or fourteen ducts, which open on the conjunctiva at its upper and outer part. The constant motion of the upper eyelid induces a continuous gentle current of tears over the surface, which carry away any foreign particle that may have been deposited on it. The fluid then passes through two small openings, termed the puncta lachrymalia (see 9 in fig. 7), into the canals; whence its further course into the lower portion of the nose is sufficiently obvious from the figure. The conjunctiva (or mucous coat) which covers the front of the eyeball, and lines the inner surface of the lids, passes down and lines the canals, sac, and duct; and is thus seen to be continuous with the nasal mucous membrane, of which it may be regarded as an offshoot or digital prolongation.
We shall conclude this sketch of the anatomy of the human eye by a brief notice of the nerves going to this organ and its appendages. Into each orbit there enters a nerve of special sense—viz. the optic nerve; a nerve of ordinary sensation—viz. the ophthalmic branch of the fifth nerve; and certain nerves of motion going to the muscular tissues, and regulating the movements of the various parts—viz. the third, fourth, and sixth nerves.
As the optic tracts from which the optic nerves originate are noticed in the article BRAIN, we shall merely trace these nerves from their chiasma or commissure forwards. This commissure results from the junction of the optic tracts of the two sides; and it is especially remarkable for the fact that it presents a partial decussation of the nervous fibres; the central fibres of each tract passing into the nerve of the opposite side, and crossing the corresponding fibres of the other tract, while the outermost fibres, which are much fewer in number than the central ones, pass to the optic nerve of the same side. In front of the commissure, the nerves enter the optic foramen at the apex of the orbit, receive a sheath or investment from the dura mater, acquire increased firmness, and finally terminate in the retina. The peculiar mode of termination of the optic nerves in the cuplike expansion of the retina, the impairment or loss of vision which follows any morbid affection of them, and the constant relation in size which is observed in comparative anatomy between them and the organs of vision, afford sufficient evidence that they are the proper conductors of visual impressions to the sensorium.
The first or ophthalmic division of the fifth or trifacial nerve sends branches to the eyeball (ciliary nerves), to the skin of the eyelids, and to the conjunctiva. That it is the nerve of ordinary sensation of the eye is sufficiently obvious from the following facts: (1) That in disease of this nerve in the human subject, it is not uncommon to find the surface of the eyeball totally insensible to every kind of stimulus (particles of dust, pungent vapours, &c.); and (2) that if the nerve be divided in the cranium (in one of the lower animals), similar insensibility results.
The most important of the nerves of motion of the eye is the third nerve, or motor oculi. It supplies with motor power the elevator of the upper eyelid, and all the muscles of the globe, except the superior oblique and the external straight muscle, and, in addition to this, it sends filaments to the iris and ciliary muscle within the eye. The application of an irritant (in vivisection experiments) to its trunk induces convulsive contraction of the principal muscles of the ball and of the iris; while paralysis or division of the trunk occasions an external squint, with palsy of the upper eyelid and fixed dilatation of the pupil. The squint is caused by the action of the external straight and the superior oblique muscles, while the other muscles are paralysed by the operation. The normal motor action of the nerve upon the iris, in causing contraction of the pupil, is excited through the optic nerve, and affords a good illustration of Reflex Action (q.v.); the stimulus of light falling upon the retina, and, through it, exciting that portion of the brain from which the third nerve takes its origin. This nerve clearly exerts a double influence in relation to vision: (1) it mainly controls the movements of the eyeball and the upper eyelid; and (2) from its connection with the muscular structures in the interior, it regulates the amount of light that can enter the pupil, and the adjustment of the eye to various distances. The fourth nerve supplies the superior oblique muscle with motor power, while the sixth nerve similarly regulates the movements of the external straight muscle—the only two muscles in the orbit which are not supplied by the third pair. Although not entitled to be termed a nerve of the orbit, the facial nerve deserves mention as sending a motor branch to the orbicularis muscle, by which the eyelids are closed.
(2) Comparative Anatomy of the Eye.—In mammals, the structure of the eye is usually almost identical with that of man. The organ is, however, occasionally modified, so as to meet the peculiar wants of the animal. Thus, in the Cetacea, and in some amphibious Carnivora that catch their prey in the water, the shape of the lens is nearly spherical, as in fishes, and there is a similar thickening of the posterior part of the sclerotic, so as to thrust the retina sufficiently forward to receive the image formed by such a lens. (See the subsequent remarks on the eyes of fishes.) Again, instead of the dark-brown or black pigment which lines the human choroid, a pigment of a brilliant metallic lustre is secreted in many of the mammalia, forming the so-called tapetum lucidum at the bottom of the eyeball, which seems (according to Bowman) to act as a concave reflector, causing the rays of light to traverse the retina a second time, and thus probably increasing the visual power, particularly where only a feeble light is admitted to the eye. The pupil, moreover, varies in form, being transversely oblong in the Ruminants and many other Herbivora, and vertically oblong in the smaller genera of Cats. These shapes are apparently connected with the positions in which the different animals look for their food. Lastly, in some mammals (e.g. the horse) there is a rudimentary third eyelid corresponding to the membrana nictitans of birds.
In birds, the eye, though presenting the same general composition as in man, differs from the mammalian eye in several important points. From our knowledge of the habits of birds (especially birds of prey), we should naturally expect that in their rapid movements they would be able readily to alter the focus between the extremes of long and short sighted vision, and the modifications we shall now proceed to notice clearly have this object in view.
In reference to fig. 8, which represents a section to allow room for a large quantity of aqueous humour, and to increase the distance between the lens and the posterior part of the retina, and thus to produce a greater convergence of the rays of light, by which the animal is enabled to discern near objects. In order to retain this elongated form, we find a series of bony plates, forming a broad zone, extending backwards from the margin of the cornea, and lying imbedded in the sclerotic. The edges of the pieces forming this bony zone overlap each other, and are slightly movable, and hence, when they are compressed by the action of the muscles of the ball, there is protrusion of the aqueous humour and of the cornea, adapting the eye for near vision; while relaxation of the muscles induces a corresponding recession of the humour and flattening of the cornea, and fits the eye for distant vision. The focal distance is further regulated by a highly vascular organ called the marsupium, or pecten, which is lodged in the posterior part of the vitreous humour (fig. 8, a). It is attached to the optic nerve at the point where it expands into the retina, and seems to be endowed with a power of dilatation and contraction; as it enlarges, from distension of its blood-vessels, it causes the vitreous humour to push the lens forwards, while, as it collapses, the lens falls backwards again towards the retina. of the eye of the owl, we see (1) that the shape of the organ is not spherical, as in mammals, nor flattened anteriorly, as in fishes and aquatic reptiles, but that the cornea is very prominent, and the antero-posterior diameter lengthened; the consequence of this arrangement being
In addition to an upper and lower eyelid, birds have an elastic fold of conjunctiva, which, in a state of repose, lies in the inner angle of the eye, but is movable by two distinct muscles, which draw it over the cornea. It is termed the membrana nictitans; it is to a certain degree transparent, for (according to Cuvier) birds sometimes look through it, as, for example, the eagle when looking at the sun. The lachrymal gland is situated as in mammals, but there is here a second gland, the glandula Harderi, which yields a lubricating secretion.
There are no very special peculiarities in the eyes of reptiles, and we therefore proceed to notice the most remarkable points presented by the eye in fishes. From the comparatively great density of the medium (water) through which the rays of light pass before they impinge upon the transparent structure of the eye of the fish, it is obvious that this organ must act as a very powerful refractive apparatus. The main peculiarity in the eye of the fish is the size, extreme density, and spherical shape of the lens, which give it such an extraordinary magnifying power that it has been employed as a simple microscope. See Brewster's Treatise on the Microscope, p. 31. But its focus being shortened in proportion as its power is increased, it is necessary that the retina should be brought near its posterior surface. For this purpose the eyeball is flattened by diminishing the quantity of vitreous humour; and this flattened form is maintained by the existence of two cartilaginous plates in the tissue of the sclerotic, which in some of the larger fishes is actually converted into a bony cup. The aqueous humour, as the cornea has here hardly any refractive power and is also flattened, is barely sufficient to allow the free suspension of the iris. The pupil is very large, so as to take in as much light as possible, but is generally motionless. Their eyes being constantly washed by the water in which they live, no lachrymal apparatus is necessary, nor does any exist; and the same remark applies to the cetacea amongst the mammals. We thus see that throughout the sub-kingdom of the vertebrata the eye is constructed according to one general scheme, with modifications to suit the mode of life of individual classes.
There is another organ present in most vertebrate animals which seems, from recent investigations, to represent an eye, though it is very doubtful whether it has the power of sight in any living animal. This is represented in mammals and birds by the pineal gland (see BRAIN); but in some lizards is placed upon the top of the head, and has the appearance of a rudimentary eye, similar in structure to that of some of the Invertebrata.
In the Invertebrata there is an immense variety in the structure of the eye where such an organ is present. There are two main types, simple and compound eyes. In simple eyes (of which the human eye itself is the most highly organised form), every degree of complexity is present, from a mere pigmented spot, with or without a rudimentary lens, to an organ nearly as complicated as that of the Vertebrata (e.g. in some of the Cuttle-fishes), with a cornea, iris, lens, and retina all well developed. In these eyes, however, almost without exception, the nerve expands behind the retina, and the percipient elements are directed towards the light; while in the vertebrate eye the opposite arrangement obtains.
Some of these organs are so rudimentary that they can have no function beyond mere perception of light; but in cases where they are sufficiently developed to admit of the perception of objects, they see, roughly speaking, as our eyes do—that is to say, a more or less accurate picture of external objects is thrown on the expansion of nerve-endings corresponding to the retina, and its direction is reversed (see below).
In the compound eyes the whole principle of the structure and perception is different. They are best developed in Insects (q.v.), and in the higher Crustaceans; but occur in a rudimentary condition in some molluscs. The surface of such an eye is divided into a number of hexagonal facets, the cuticle of each generally forming a minute lens. Beneath each facet is a transparent rod, surrounded and separated from those adjacent to it by pigment, and leading inwards to the retinula, a group of cells in connection with the terminal fibrils of the optic nerve. In most familiar insects they form two hemispherical masses on the sides of the head. In some ants there are only fifty facets in each eye; in the house-fly about 4000; in some beetles as many as 25,000. It is probable that in these eyes only the rays of light which fall upon a particular facet exactly, or very nearly, in the direction of the transparent rod beneath it can reach the corresponding nerve-fibre, and that other rays are absorbed by the pigment around the rod. Each percipient element therefore receives light only from a very small portion of the field of vision, and the picture is a mosaic, each element of which is furnished by a different facet of the eye. The picture has obviously the same position as the objects it represents, instead of being inverted as in a simple eye. Most insects have simple as well as compound eyes; but the latter have by far the most perfect vision.
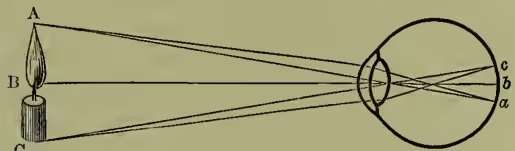
(3) We may now proceed to the consideration of the uses of the various parts of the eye. Assuming a general knowledge of the ordinary laws of geometrical optics (see OPTICS, LENS, &c.), we shall trace the course of the rays of light proceeding from any luminous body through the different media on which they impinge. If a luminous object, as, for example, a lighted candle, be placed in front of the eye, some of its rays fall upon the cornea, and are in part reflected, giving to the surface of the eye its beautiful glistening appearance; in part refracted or converged by it, to enter the aqueous humour, which exerts no perceptible effect on their direction. Those which fall on and pass through the outer or circumferential part of the cornea are stopped by the iris, and are either scattered or absorbed by it; while those which fall upon its more central part pass through the pupil, and are concerned in vision. In consequence of its refractive power, the rays passing through a somewhat larger surface of the cornea than the pupil are converged so as to pass through it and impinge upon the lens, which, as its refractive index is much greater than that of the aqueous and vitreous humours, by the convexity of both its surfaces very much increases the convergence of the rays passing through it. They then traverse the vitreous humour, whose principal use appears to be to afford support to the expanded retina, and are brought to a focus upon that tunic, forming there, if the eye be adjusted for the distance from which the rays proceed, an exact but inverted image of the object.
This inversion of the image may be easily exhibited in the eye of a white rabbit or other albino animal, after removing the muscles, &c. from the back part of the globe. The flame of a candle (A, B, C, fig. 10) held before the cornea may be seen inverted at the back of the eye (a, b, c), increasing in size as the candle is brought near, diminishing as it retires, and always moving in a direction opposite to that of the flame.
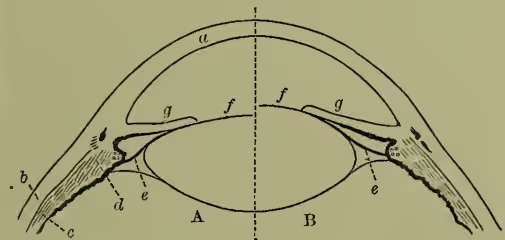
The adjustment of the eye for distinct vision at different distances, or accommodation, must next be considered. The normal eye in the position of rest is adjusted to see objects at a distance (practically all objects at 20 feet or more are seen with equal clearness): to see a near object (at 10 inches, say) a distinct effort is required, and when the effort ceases the object at once appears blurred. Careful observations and measurements by means of a suitable instrument (Ophthalmometer) of images reflected from the three principal refracting surfaces of the eye (cornea, anterior and posterior surfaces of crystalline lens) have shown that during accommodation for a near object (1) the position and curvature of the cornea remains unchanged; (2) the anterior surface of the crystalline lens approaches the cornea and becomes much more convex; (3) the posterior surface does not change its position, but becomes very slightly more concave. Accommodation, then, depends upon change of shape of the crystalline lens. The true explanation of the mechanism by which this is effected was first given by Helmholtz. The ciliary muscle, as already stated, has its fixed attachment all round within the sclerotic close to the margin of the cornea; and passes outwards and backwards to the anterior part of the choroid, close to the ciliary processes. When it contracts, therefore, it draws these structures inward; and with them the outer attachment of the suspensory ligament of the lens. The tension of this membrane is thus relaxed, and the elastic lens, whose form as well as position is controlled by it, is allowed to assume a more spherical shape. When the ciliary muscle ceases to contract, the converse takes place, and the lens is again flattened as the suspensory ligament and lens capsule become more tense. With the contraction of the ciliary muscle is always associated a contraction of the circular fibres of the iris, diminishing the size of the pupil; and when the ciliary muscle relaxes, the pupil enlarges again. This change, though of much less importance than the change in shape of the lens, is much more easy to observe.
Change of adjustment requires a short but measurable time; that from distant to near vision requires a little longer time than the converse; the former from a little over one to two seconds, the latter about one second.
As age advances, the power of accommodation steadily and quickly diminishes, not because the ciliary muscle gets weaker, but because the lens becomes less elastic. This change begins during youth, but is not commonly noticed before middle life. At ten years of age an object can be seen distinctly at less than 3 inches; at twenty, not nearer than 4 inches; at about forty-five, not nearer than 10 inches; at sixty, not nearer than 3 feet. After seventy-five, the lens is so unyielding that accommodation is altogether lost. When the shortest distance at which distinct vision is possible approaches that at which reading or work is usually attempted, the failure of accommodation begins to attract attention, and spectacles have to be resorted to to compensate for it. This condition has received the name of presbyopia or old sight, but must be clearly understood to be perfectly natural after the age of forty-five, and in no way to imply defect or weakness of the eyes.
The eye, regarded as an optical instrument, has numerous imperfections: the more important of these must be mentioned.
Spherical aberration (see LENS) is in part avoided by the iris, which, acting as a diaphragm, cuts off all but the central pencil of rays; in part by the forms of the refracting surfaces, which are not truly spherical, but ellipsoidal or hyperbolical—i.e. more curved at the centre than elsewhere; in part by the constitution of the lens (see above). What remains is, like chromatic aberration, for which no correction seems to exist, too slight to be perceptible.
Regular Astigmatism (q.v.) is present in almost all eyes, but is generally so small in amount as to be of no importance.
Imperfect Transparency of Media.—The stellate arrangement of the lamellæ of the lens is the cause of the rayed (or, as we say, star-shaped) appearance of a point of light. Muscae volitantes, the clear threads or strings of beads often seen in looking at a bright surface flitting about when the eye is moved, are due to the shadows of the minute fibres and corpuscles naturally present in the vitreous humour.
(4) We must now consider how the image formed in the back of the eye by the dioptic media gives rise to vision. It is the retina, and only that part of it known as the layer of rods and cones (see fig. 5), which is directly affected by light.
Let two marks be made on a sheet of paper about 3 inches apart horizontally (a cross and a round mark to the right of it). Close the left eye, and holding the paper about a foot from the face, look steadily at the cross; the circle is also visible. Now bring the paper gradually nearer, keeping the right eye fixed upon the cross. The circle soon disappears; but becomes visible again when the paper is brought still nearer the eye. The blind spot in which the circle becomes invisible is the entrance of the optic nerve; hence we know that the nerve-fibres themselves are not sensitive to light. Further proof of this is given by Purkinje's figure, which is easily perceived as follows: Take a candle in a room otherwise dark, and holding it a short distance in front and to the outer side of one eye, move it from side to side, looking straight forward. A set of branching dark lines, the shadows of the retinal blood-vessels, will be seen (see fig. 4). These could not be perceived unless the sensitive portion of the retina lay behind the blood-vessels, which the nerve-fibre layer of the retina does not.
Stimulation of the retina, however it may be caused, gives rise to the sensation of light. Thus, slight pressure on one side of the eyeball causes an appearance of flashes of light towards the opposite side. A sudden blow on the eye, or the indirect shock to it of a fall on the head, makes one 'see stars.' Electric currents passed through the eye similarly cause a sensation of bright light. But true vision is only caused by rays of light falling upon the retina.
In what way light affects the layer of rods and cones we do not know. Probably it produces some chemical change, which leads to stimulation of the nervous elements. A substance called visual purple or rhodopsin has been found in the outer segments of the rods of some mammals, which is bleached on exposure to light, and restored in darkness. Photographic pictures of bright objects have even been obtained in eyes of rabbits, &c. by means of it. But as it is absent in the most sensitive portion of the human retina, it cannot be the chief factor in the production of vision.
The fovea centralis (see fig. 1) is the part of the retina where vision is most acute: as cones only are present here, it is clear that they are more delicately adjusted for their function than the rods, which greatly preponderate at other parts of the retina. When the eye looks straight at an object (or in technical language fixes it), its image falls upon this part of the retina. In direct vision, as this is called, two black marks on a white ground are distinguished as separate when the interval between them subtends an angle of about one minute at the eye. It is found by calculation that this angle, prolonged to the back of the eye, pretty nearly corresponds to the distance between two adjacent cones at the fovea centralis. The vision at other parts of the retina (indirect vision) is very much less acute, and less capable of accurate measurement. We have only to fix steadily one letter in a page of ordinary print to satisfy ourselves in how small an area we can see sufficiently distinctly to make out words without moving the eyes. The field of vision, or whole space within which objects are perceived by an eye while it is fixed upon one point, is very much wider, extending in each eye to more than 90 degrees from the fixation point or centre to the outer side, and rather less in other directions. Colour-vision is also most distinct at the centre of the field; and it is found that it diminishes more rapidly towards the outer portions than light-vision, so that near the limits of the field colours cannot be recognised.
There must be a certain amount of light for the purpose of vision. Every one knows that it is difficult and painful to discern objects in a very faint light; and, on the other hand, that on suddenly entering a brilliantly lighted room from the dark, everything appears confused for one or two seconds. There is, however, a gradual adaptation of the retina to different amounts of light. Persons long immured in dark dungeons acquire the power of distinctly seeing surrounding objects; while those who suddenly encounter a strong light are unable to see distinctly until the shock which the retina has experienced has subsided, and the iris has duly contracted. In protecting the retina from the sudden effects of too strong a light, the iris is assisted by the eyelids, the orbicular muscle, and to a certain extent by the eyebrows. Moreover, the dark pigment of the choroid coat acts as a permanent guard to the retina, and where it is deficient, as in albinos, an ordinary light becomes painful, and the protective appendages, especially the eyelids, are in constant use.
The persistence during a certain time of impressions made on the retina facilitates the exercise of sight. Such persistent impressions are called after-images. A momentary impression of moderate intensity continues for a fraction of a second; but if the impression be made for a considerable time, or be very intense, it endures for a longer period after the removal of the object. Thus, a burning stick, moved rapidly in a circle before the eyes, gives the appearance of a continuous ribbon of light, because the impression made by it at any one point of its course remains on the retina until it again reaches that point. It is owing to this property that the rapid and involuntary act of winking does not interfere with the continuous vision of surrounding objects; and, to give another illustration of its use, if we did not possess it, the act of reading would be a far more difficult performance than it now is, for we should require to keep the eye fixed on each word for a longer period, otherwise the mind would fail fully to perceive it. However great may be the velocity of a luminous body, it can always be seen; but if an opaque body move with such rapidity as to pass through a space equal to its own diameter in a less time than that of the duration of the retinal impression, it is altogether invisible; and hence it is, for example, that we cannot see bullets, &c. in the rapid part of their flight. In these cases the after-image is of similar brightness and colour to the original impression, and is known as a positive after-image. When the stimulation of the retina is very strong, or the retina itself in a very sensitive condition—e.g. in certain morbid states of the system and in twilight, a negative after-image appears, in which the bright parts of the original impression appear dark and vice versa. An image of this kind may persist for some seconds or minutes or even longer. This physiological phenomenon has probably given origin to many stories of ghosts and visions. Thus, if a person has unconsciously fixed his eyes, especially in the dusk, on a dark post or stump of a tree, he may, on looking towards the gray sky, see projected there a gigantic white image of the object, which may readily be mistaken for a supernatural appearance. The phenomenon is easily seen on looking away from a bright window after directing the eyes to it for some time, when the bars appear as bright lines on a dark ground. Negative after-images are always of the complementary colour to that of the object. Thus, the image left by a red spot is green; by a violet spot, yellow; and by a blue spot, orange.
(5) Each eye can be moved from its ordinary position, looking straight forward, through an angle of nearly 60 degrees downwards, and of 35 to 45 degrees in other directions. But one eye never moves without the other. Two series of associated movements have to be distinguished: movements of both eyes in the same direction, and movements which converge the eyes, or bring the corneæ of both eyes towards each other. When a near object is looked at, the movement of accommodation is associated with a proportionate contraction of the internal recti of both eyes, so as to direct the visual axis, or in other words the fovea centralis, of each towards the object.
If we suppose the retinæ of the two eyes to be placed in contact, so that the foveæ centrales and the vertical meridians correspond, then all points which lie together in the two retinæ are called corresponding points, and have the property that simultaneous stimulation of both gives rise only to a single impression. An object whose image falls upon corresponding points thus appears single; otherwise it appears double. Hold up two fingers in line in front of the face. When the nearer one is looked at, it is seen single, but the farther appears double and somewhat out of focus; when the farther is looked at, it appears single, and the nearer is similarly doubled and blurred. Generally speaking, images of the great majority of the objects in the field of vision of both eyes must fall on non-corresponding points of the two retinæ; but as the attention is generally directed to the images of the object for which the eyes are accommodated, and as these, falling upon the foveæ centrales, are much the most distinct, the double vision of other objects is seldom noticed.
In the case of near objects, however, something more is needed to explain single vision. For example, take the case of a solid object. The two eyes, looking from different points of view, receive quite different images; the right eye sees more of the right side, the left eye more of the left. It is impossible that the images of each point of the object can fall upon accurately corresponding points of the two retinæ. Yet the appearance presented is that of a single object clearly defined. In this case then there must be in the brain-centres a power of combining in a single picture images which do not accurately correspond.
Various topics which the reader might perhaps have expected to find noticed, such, for instance, as 'the appreciation of solid forms by the sense of vision,' 'correct vision with an inverted image on the retina,' &c., which belong fully as much to metaphysics as to physiology, are discussed in the article on VISION. We may also refer those who desire information on these points to Professor Bain's treatise on The Senses and the Intellect.
For the anatomy of the eye, see Quain or other standard work. Lubbock in The Senses of Animals gives a concise account of the chief types of eyes in the Invertebrata. Helmholtz's Physiological Optics is the classical work on the optical aspects of the eye. The larger works on human physiology—e.g. Foster, Landois and Stirling—may also be consulted.
DISEASES AND INJURIES OF THE EYE, as might be expected from the delicate and complicated structure of the organ, are very numerous. But as the position of the eye and the transparency of its dioptric media give exceptional facilities for their detection and study, they are more thoroughly understood than those of any other organ. Only the most common and important can be referred to here.
Diseases of Conjunctiva are mainly different forms of inflammation, or conjunctivitis. (a) Simple or Catarrhal Conjunctivitis may be acute or chronic. In the former case, it is commonly called 'cold in the eye.' The white of the eye is more or less reddened, and there is an increased discharge of gummy substance, causing the lids to cohere during sleep; a sensation is experienced as of sand or dust in the eyes, and there is a little increased sensitiveness to light. The acute form generally subsides in a few days without leaving any ill effects, unless improperly treated; the chronic form is often obstinate. The common popular treatment—viz. tying wet cloths or poultices over the eye, cannot be too strongly condemned; it may produce temporary relief of irritation, but aggravates the inflammation, and is very apt to lead to ulceration of the cornea. A mild astringent lotion should be used thrice or oftener in the day (cold tea; boric acid 10 grains, alum 3 grains, to the ounce of water); and a little simple ointment or fresh butter applied to the lids at bedtime to prevent their becoming glued together. The chronic form often requires stronger remedies, but they should not be used except under medical advice. (b) Purulent Conjunctivitis resembles the last, but is very much more severe, and highly dangerous. In its most characteristic forms it is known as gonorrheal ophthalmia, and ophthalmia neonatorum (eye inflammation of new-born children). To the latter variety about one-third of the blind persons in Europe owe their loss of sight. It is produced by inoculation of the eye with certain irritating discharges; and the discharge from an affected eye will infect any other eye with which it comes in contact. The conjunctiva becomes intensely red and swollen, and the lids partake in the swelling so that they cannot be opened; there is severe burning pain, and after two days or more a profuse discharge of matter. The danger to sight is due to the fact that the cornea is extremely apt to be destroyed, wholly or in part, before the inflammation subsides. In infants the disease usually begins on the third day after birth, and is, as a rule, less severe than in the adult, but unfortunately is often overlooked, or regarded as of no importance till irreparable mischief has been done. Scrupulous cleansing of the eyes immediately after birth, preferably with corrosive sublimate lotion (1 grain to 8 ounces) is the best preventive. When the disease has commenced, very frequent removal of discharge and hourly washing with boracic or corrosive sublimate lotion should be resorted to. But all such cases should at once be put under the charge of a medical man. (c) Pustular or Phlyctenular Conjunctivitis is a form of inflammation very frequent in children, much less so in adults. It is an indication of a lowered state of the general health, and its treatment must include fresh air and light, good food, and cod-liver oil or some other strengthening medicine. The inflammation does not extend all over the white of the eye, but is localised in one or more sections of it, and is most intense near the margin of the cornea, where one or more small rounded blebs or pimples may be seen. It is often accompanied in children by extreme tenderness to light; but the tendency to this is aggravated by a bandage or darkness. The local treatment should be bathing with boracic acid or some other mild astringent lotion; but, unless the case be very mild, a medical man should be consulted. (d) Granular Conjunctivitis, or trachoma, is an exceedingly chronic and intractable disease. It is sometimes called Egyptian ophthalmia, having been extremely prevalent in the French army in Egypt in 1798. In Europe it is most common among the Jews and the Irish, but is often troublesome in industrial schools and similar institutions. It is encouraged by overcrowding, bad ventilation, and other unfavourable hygienic conditions, and is undoubtedly somewhat contagious. It is characterised by numerous distinct semi-transparent elevations on the conjunctiva of the lids, chiefly the upper. It often lasts for months or years, and is chiefly dangerous on account of the shrinking of the conjunctiva produced by it, which leads to trichiasis, Ectropion (q.v.), and opacity of the cornea. It should always be treated by a skilled medical man. (e) In Diphtheritic Conjunctivitis there is a 'false membrane' formed on the conjunctiva, as in Diphtheria (q.v.) in other situations. It is happily rare in Britain.
Diseases of the Cornea.—The most common and important are inflammations associated with ulceration—i.e. destruction of some of the corneal substance. This is replaced when healing takes place by imperfectly transparent tissue, and results very frequently in great impairment of vision (irregular Astigmatism, q.v.), even where no obvious mark remains. The appearances, symptoms, and appro- priate treatment of different forms and stages of corneal ulceration are extremely various, and cannot profitably be discussed here. Skilled medical advice should always be obtained. It must suffice to say that the eyes should be rested, shaded from light, and bathed, generally with boracic or corrosive sublimate lotion. Poulticing or tying up the eyes should never be resorted to unless under a doctor's orders, as it is usually still more mischievous than in conjunctivitis.
In one form of inflammation of the cornea, called interstitial, there is an appearance all over it of great haziness or even complete opacity, but without breach of surface. It occurs usually in boyhood or girlhood, and though alarming in appearance and tedious, generally results in complete recovery. Mr Jonathan Hutchison first pointed out that it is usually a manifestation of congenital syphilis.
The sclerotic is comparatively seldom affected by disease, probably on account of its slight vascularity and comparatively low vitality.
The iris is liable to inflammation (iritis), characterised by severe deep-seated pain, redness of the white of the eye, contracted pupil, and much dimness of sight. The inflammation, if unchecked, produces adhesion between the posterior surface of the iris and the anterior capsule of the lens, which may permanently interfere with vision, or even lead ultimately to complete loss of sight. Local treatment at the early stage by Atropia (q.v.) dilates the pupil and prevents the formation of adhesions. Unless the result of injury, iritis usually depends on constitutional causes, especially syphilis and rheumatism, and treatment of these is of prime importance for its cure. Medical aid should be sought at once; for atropia, which is most beneficial in iritis, is disastrous in glaucoma, a disease which sometimes resembles it in many of its symptoms.
The chief disease of the lens is opacity, or Cataract (q.v.); it may also be displaced or dislocated, either from an anomaly in its development, or as the result of injury.
Diseases of the deeper structures of the eye (choroid, vitreous humour, retina and optic nerve) usually require for their recognition the use of the Ophthalmoscope (q.v.). Generally speaking, they are associated with little or no pain, and attract the patient's attention in consequence of the dimness of vision they produce. They are much less amenable to treatment in most cases than affections of the more superficial parts.
Inflammation and atrophy of the choroid occur in several forms; the most distinct are those occurring in syphilis, in old age, and in connection with high degrees of short-sightedness (progressive myopia, see below).
The vitreous humour rarely if ever becomes diseased, except in consequence of changes in the ciliary body or choroid. The abnormal condition generally manifests itself in more or less opaque threads or films, which move with the movements of the eye, and appear to the patient as clouds or dark lines interfering with vision, much more large and distinct than the 'muscæ volitantes' present in the normal eye.
The retina may be the seat of hemorrhage or of inflammation in many forms of disease. The most common and characteristic retinitis is that associated with Bright's disease (q.v.), which is almost always of very serious import. Its main artery may become blocked by a plug carried into it from the heart or elsewhere (Embolism; see ARTERIES, DISEASES OF), an accident which causes sudden and usually almost complete loss of sight. Not unfrequently, too, the retina becomes detached from the choroid, either as the result of disease or injury, and floats in the vitreous chamber in front of its normal position, a condition greatly interfering with sight, and most difficult to improve.
The optic nerve may become inflamed (optic neuritis), most commonly in consequence of an inflammation or tumour of the brain or its membranes. It may degenerate (optic atrophy) either after inflammation or independently of it. In the latter case, however, as well as the former, there is in the great majority of instances some disease of other parts of the nervous system (brain or spinal cord).
There are two diseases chiefly affecting the deeper parts of the eye which it is desirable to describe at some length, as their course is often insidious, and their results when not recognised early, most disastrous, while timely interference is often signally successful in preserving the sight. These are glaucoma and sympathetic ophthalmia.
Glaucoma occurs most commonly during or after middle life, frequently in persons whose eyes are hypermetropic (see below). It may come on with such suddenness and intensity that vision is lost in a few hours, or its course may extend over years. Always, however, if unchecked, it tends to progress till sight is destroyed. Both eyes are usually affected, but often one long before the other. In many cases there are premonitory symptoms, consisting in temporary attacks of cloudiness of vision, during which the patient, when looking at a light (e.g. a gas or candle flame), sees it surrounded by coloured rings or halos. During this 'premonitory stage,' the vision is perfectly normal between the attacks; but they become more frequent and prolonged, till it is permanently impaired. Variability of the symptoms is usually a characteristic feature in all stages of the disease. Often in the later phases, and always in acute and severe cases, much pain is experienced in and around the eye affected. The pupil is large and immobile; the iris and lens farther forward than normal; the cornea more or less hazy; and some of the blood-vessels of the white of the eye larger and more visible than they should be. The most important sign of the disease, and the feature on which many of its characteristics depend, is increased hardness of the eyeball, owing to increase of its contents. The exact cause of this increased hardness is not fully understood, nor the way in which some of the symptoms observed depend upon it; but it varies with the symptoms, being always more marked when the pain and dimness are at their worst. Chronic insidious cases are often mistaken for cataract, though the use of the ophthalmoscope readily distinguishes between the two conditions; in the most acute cases, the headache, sickness, and general disturbance of the system is sometimes so severe that the condition of the eyes is overlooked, and the disease is looked upon as a 'bilious attack' till the vision is hopelessly destroyed.
The disease was regarded as absolutely hopeless till Von Graefe, in 1857, proved that the removal by operation of a portion of the iris of a glaucomatous eye might arrest the process. This proceeding (iridectomy), though by no means uniformly successful, does good in the majority of cases, and has been of enormous benefit. But if too long delayed, it is of no avail for the restoration of vision.
It is of great importance that atropin or belladonna should not be applied to an eye with any tendency to glaucoma, as they aggravate the disease, and sometimes even produce it. Eserin, the active principle of the Calabar bean, has an action on the eye antagonistic to atropin, and can often keep glaucoma in check, though it rarely cures it. Pilocarpin, the active principle of Jaborandi, has a similar action.
Sympathetic Ophthalmia is the name given to a form of inflammation, chiefly of the iris and ciliary body, occurring in an eye previously healthy in consequence of disease or injury of the other. Almost, if not quite, invariably the eye first affected has had its coats (cornea or sclerotic) perforated; and the process in the second eye may begin at any time, from a fortnight to many years after this occurrence. It is an extremely insidious disease, sometimes quite painless; but also extremely dangerous, for it often leads to total loss of sight. The early symptoms are watering, tenderness to light, and dimness of sight, especially of near objects. When it begins, there is almost invariably irritability and tenderness to touch in the eye which is the origin of the disease. It can be absolutely prevented by early removal of the eye first affected; but if this be delayed till the inflammation has begun in the second eye, it may be useless. An eye which has received a perforating wound, particularly in the 'ciliary region'—i.e. just outside the cornea—may therefore at any subsequent period become a source of danger to the other eye; and if its vision is destroyed there can be no doubt that it should be removed. Even if some useful sight is retained, this may sometimes be desirable; but at all events, every one who has suffered from such an injury to one eye should know that the slightest symptoms of irritation or failure of sight in the other should at once lead him to seek skilled advice. Recent researches have rendered it probable that this form of inflammation is caused by micro-organisms, though this is not quite definitely established.
Errors of refraction are those defects in the dioptric media of the eye which, without diminishing their transparency, interfere with the formation of a retinal image in the normal way. Astigmatism (q.v.) has already been noticed; presbyopia is the failure of accommodation natural to age (see above). It remains to describe myopia, or short-sightedness, and hypermetropia, or long-sightedness. In most cases the condition of both eyes is alike, or nearly so; but exceptionally there is a considerable difference between them (anisometropia).
The knowledge of this branch of the subject was first systematised and placed on a satisfactory basis by Donders (1818-89), a distinguished Dutch physician and physiologist, professor of Physiology at Utrecht, in his work on Anomalies of Accommodation and Refraction of the Eye (Eng. trans. pub. by Sydenham Society, 1866).
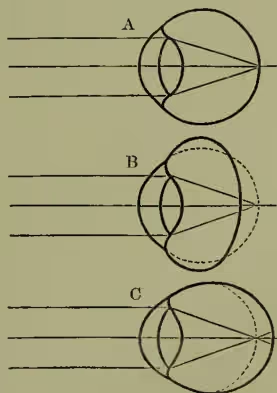
The normal eye in the position of rest is adjusted for parallel rays—i.e. for a distant object, and by means of the accommodation can be focused for a near object. The short-sighted eye at rest is adjusted for divergent rays—i.e. for a near object; accommodation enables it to focus for a still nearer object, but it can make no change enabling it to see clearly beyond its 'far point'—i.e. that for which it is adjusted at rest. The long-sighted eye at rest is adjusted for convergent rays, which do not occur in nature; accommodation enables it to focus parallel rays (from distant objects), or divergent rays (from near objects), but not to see so near as a normal eye of the same age.
These defects generally depend on an abnormality in the length of the antero-posterior diameter of the eyeball; in short-sighted eyes it is greater, in long-sighted less than the normal (see fig. 12). They can be corrected by the use of suitable glasses; in short-sighted eyes concave lenses are used, which render the rays of light falling upon them more divergent; in long-sighted eyes convex lenses, which render the rays less divergent or convergent.
Loss of accommodation occurs with the progress of years in such eyes, just as in normal ones, though the effects are somewhat different. The short-sighted eye continues to be able to see near at hand without spectacles; but, contrary to the popular belief, has no other advantage over the normal eye as age advances, for vision of distant objects does not improve. The long-sighted eye in time loses the power of seeing even distant objects without spectacles; and the higher the degree of long-sightedness the earlier the age at which this occurs.
An abnormal shape of the eye, on which these 'errors of refraction' usually depend, is frequently hereditary, and is incurable; it usually remains stationary after early adult life, but in some cases of myopia, where it is associated with disease of the choroid, tends to become worse (progressive or malignant myopia). The object of treatment must be to counteract, so far as possible, the inconvenience resulting; and this can generally be done by the use of spectacles or eyeglasses. No general rules can be laid down as to their use, as much depends not only on the degree of the abnormality, but on the age and occupation of the individual. If glasses conduce to comfort and to the preservation of the sight, no mere regard for appearance should prevent their being worn.
Diseases of the Eyelids.—A stye is practically a minute Boil (q.v.) formed in the eyelid, and discharging at its margin. It should be fomented frequently with hot water till it bursts. Constitutional treatment is often desirable, as styæ often occur, like boils, in groups or series.
Small rounded swellings (tarsal cysts) often form under the skin of the lids, owing to obstruction of the duct of a Meibomian gland. They are usually painless, but require for their cure the evacuation of their contents through a puncture on the inner surface of the lid.
A form of Eczema (q.v.) often occurs at the margin of the lids, called blepharitis, most commonly in delicate children. It can usually be readily cured if attended to in time; but if neglected, as it too often is, leads to destruction (blear eyes) or misdirection (trichiasis) of the eyelashes, and much subsequent trouble. It is characterised by redness and ulceration of the edges of the lids, usually masked by crusts adhering to the lashes. Frequent removal of these, with the daily application of a stimulant ointment (e.g. yellow oxide of mercury, 8 grains to the ounce of simple ointment), and the use of tonics generally effect a cure. Inversion (Entropion, q.v.) and eversion (Ectropion, q.v.) of the margins of the lids, and misdirection of the eyelashes (trichiasis), so that they rub against and irritate the cornea, are troublesome affections, usually requiring operation for their removal.
Diseases of the Lachrymal Apparatus.—A 'watery eye' (epiphora), when no irritating affection of the eye itself is present, usually proceeds from stricture of the nasal duct, or some other cause, which prevents the tears from discharging by their natural channel into the nose. The condition can be remedied in most cases by slitting up the canalic- ulus (see fig. 7), and passing graduated probes through the duct to restore its patency. If unattended to, it generally leads sooner or later to abscess of the lachrymal sac, with much swelling and pain.
Injuries.—In no part of the body is there so often great disproportion between the severity of an injury and the amount of pain and irritation it occasions. A penetrating wound sometimes causes less discomfort than a mere particle of sand beneath the eyelid. Any wound or blow affecting the eye, therefore, particularly if it interfere at all with the sight, should be seen by a doctor as speedily as possible. Substances thrown against the eye may injure it. Quicklime is rapidly destructive to the eye, slaked lime and mortar less so. When one of these, or any other alkaline caustic, has got into the eye, diluted vinegar should at once be used to neutralise it. If it is oil of vitriol (sulphuric acid) or another acid that has been the cause of the injury, a weak solution of soda may be used in the first place to neutralise the acid. After this, sweet oil is the best thing to introduce, until the surgeon arrives. In gunpowder explosions near the eye, besides the burn, the particles are driven into the surface of it, and will cause permanent bluish stains over the white of the eye, unless they are carefully removed at the time. When chips of glass, stone, &c. are driven into the interior of the eye, there is little hope of its being saved from destructive inflammation, though fragments of iron and steel are sometimes removed by means of a strong electromagnet, with a successful result. In these and all other penetrating wounds—i.e. those where the cornea or sclerotic is broken through, the possibility of subsequent sympathetic ophthalmia in the other eye must be borne in mind. When only partially sunk into the cornea, as is often the case with sparks of cinder or iron, &c., or 'fires,' as they are called, the rubbing of the projecting part on the eyelid causes great pain, and the surgeon has not much difficulty in removing them. Most commonly these, or other 'foreign bodies,' as particles of dust, sand, seeds, flies, &c., when not speedily washed away by the tears, merely get into the space between the eyeball and the lids, almost always concealed under the upper, as it is the larger, and sweeps the eye. They cause great pain, from the sensitiveness of the papillary surface of the lid, and of the cornea over which they are rubbed by its movements, soon excite inflammation, and their presence, as the cause, is apt to be overlooked. The lid must be turned round to find them. To do this, pull the front or edge of the lid forward by the eyelashes, held with the finger and thumb, and at the same time press down the back part of the lid with a small pencil or key, directing the patient to look downwards. The lid will readily turn round, when the body may be seen about its middle, and may be removed with the corner of a handkerchief. Another plan, which the person himself may try, is to pull forward the upper lid by the eyelashes, and push the lashes of the lower lid up behind it, when the foreign body may be brushed out. After the bodies are removed, a feeling as if they were still there may remain for some time. See BLIND, COLOUR-BLINDNESS.
ARTIFICIAL EYES are worn for the sake of appearance in cases where, as the result of disease or injury, an eye has either been totally lost, or rendered unsightly. They are, moreover, distinctly advantageous in cases where a gaping socket is liable to irritation by dust, cold winds, &c. They cannot be used unless the size and prominence of the eyeball is at least somewhat diminished. Few surgeons in Britain recommend them to be worn unless the eyeball is either entirely removed (enucleation), or has the front part removed (abscission), or all the contents extracted (evisceration); for the artificial eye is apt to cause irritation of the sensitive anterior portion of the globe, and may lead to the development of sympathetic ophthalmia (see p. 515). Enucleation is the most certain means of preventing this; but the other operations named above allow of better movement, and give a more natural appearance to the eye.
An artificial eye consists of a thin shell, usually of enamelled glass, coloured to present as nearly as possible the same appearance as the visible part of the normal eye. Quite recently Celluloid (q.v.) has been used instead of glass, and is said to last better, as its surface is not affected by the secretions; while it has the advantages that it is not brittle, and can easily be pared to fit the socket accurately. To obtain a satisfactory result, it is necessary either to have the eye specially made, or to be able to select from a very large stock; as colour of iris, size of pupil, tinge of sclerotic, as well as curvature of surface and form of margin, must be adapted to the particular case. They are therefore to be got to most advantage in large cities, such as London or Paris.
The eye must not be worn continuously, but removed each night and replaced in the morning. It is slipped in under the lids, which hold it in position. Even when the globe has been entirely removed, the muscles, by their attachment to the tissues remaining in the orbit, usually effect movements in the same direction, though not of the same extent, as those of the normal eye; and it is often difficult for any but a practised observer to detect to what the difference between the two is due. A single glass eye can rarely be worn more than a year without being polished, for the surface becomes roughened by the action of the tears, &c., and irritates the lids as they rub over it. The wearing of a glass eye therefore means an expenditure of at least one or two pounds a year, and is thus out of the power of many poor people to whom it would otherwise be an advantage.