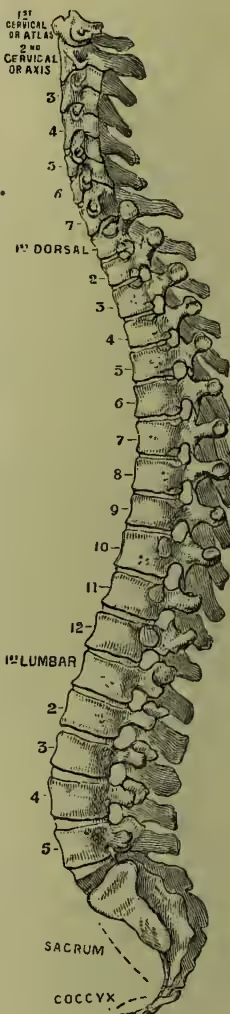
Spinal Column and Spinal Cord. The spine or spinal column is the most important and characteristic part of the Skeleton (q.v.) of the highest division of the animal kingdom. It is composed of a series of bones placed one above, or in front of another, and called vertebræ; and hence these animals, having this distinguishing characteristic in common, are all included in the term Vertebrates. The vertebræ vary greatly in number in different animals, and even in members of the same class, and the number bears no apparent relation to the other organs of the animal. Moreover, in their shape they differ extremely even in different parts of the same spine, in accordance with their special functions. In man the number of vertebræ which collectively form the spinal column is 7 in the neck (cervical vertebræ), 12 in the back (dorsal vertebræ), 5 in the loins (lumbar vertebræ), all of which are capable of being detached from one another, and are termed true vertebræ; and 5 vertebræ ossified together and forming the sacrum, and 4 or 5 similarly united forming the termination of the column, and constituting the bone called the coccyx, which are known as false vertebræ. However long or short the neck may be, every mammal has 7 cervical vertebræ, excepting the three-toed sloth which has 9, and the sea-cow which has 6. In the other regions of the spine no such uniformity exists. Each vertebra is attached to the two between which it lies by numerous strong and more or less elastic ligaments, and between each pair of vertebræ there is interposed a lenticular disc of fibro-cartilage, which acts as a buffer. By these arrangements the spinal column is rendered highly elastic, the communication of jars or shocks is prevented, and a very considerable general range of movement permitted, although the motion between any two adjacent vertebræ is slight. The elasticity of the column is further increased by the component vertebræ being arranged in curves instead of being placed perpendicularly. The curves should be exactly in the antero-posterior direction, any well-marked lateral deviation from the perpendicular being abnormal: but a very slight lateral curvature with the convexity to the right may often be detected in the upper and middle parts of the back, and is supposed to be dependent on the more frequent use and greater strength of the right arm as compared with the left. From their position they are termed the cervical, dorsal, lumbar, and pelvic curves. The dorsal and pelvic curves have their concavities in front, and thus enlarge the spaces in which the thoracic and pelvic viscera are contained; the two other curves are convex anteriorly, and thus afford support to the parts above them. The upper three curves are so arranged that their cords are in the same vertical line in the erect position of the body, and this vertical line corresponds with the line of gravity of the head. The cause of these curves is to be sought for partly in the shape of the vertebral bodies, and partly in that of the intervertebral substance. Amongst the uses of these curves it may be mentioned (1) that they enable the spine to bear a greater vertical weight than it could otherwise maintain; it is calculated that nine times as great a vertical force is required to bend it as if it had been straight; (2) that they facilitate the movements of the body, especially in the act of running; and (3) that they are so disposed as to protect the cord in movements of the spine. Similar curves are seen in the spine of other mammals (see ANTHROPOID APES), though the degree of flexure is liable to great deviations. The lumbar curve, which has especial reference to the erect position, is always much less marked than in man.
The vertebral canal formed by the apposition of the spinal foramina or neural arches, and containing and protecting the spinal cord, varies in its size at different parts of the column. It is largest in its antero-posterior diameter in the neck and loins (measuring at the last lumbar vertebra of an inch), where the antero-posterior movements of the spine are greatest, and where the cord is least closely attached to the vertebræ; while in its lateral diameter it is greatest at the atlas, where it measures nearly an inch and a half. A transverse section of the canal is nearly circular through the greater part of the back. The intervertebral foramina through which the nerves emerge vary in shape and position in different parts, but are always of sufficient size to prevent injurious pressure on the nerves during movement of the spine; and in the dorsal region, which is the ordinary seat of angular curvature, the nerves are so protected by bony arches that they may escape injury, even when the bodies of several dorsal vertebrae have been destroyed by ulceration.
The spinal cord is that part of the central nervous axis which is contained within the vertebral or spinal canal. In man it extends from the foramen magnum, where it becomes continuous with the medulla oblongata, as far down as the lower border of the first lumbar vertebra. Below this point it is continued as a narrow thread containing little nervous matter, the filum terminale. The cord is, like the brain, encased in a triple sheath of membranes, the pia, arachnoid, and dura mater, the last two of which are less closely opposed to the cord and the vertebral column than they are to the brain and the cranium. The cord is a somewhat flattened cylinder or column of a whitish colour. It is divided into two lateral halves by an anterior median fissure and a posterior median septum. The former is less deep but wider than the latter, which is merely a process of pia mater. From each side of the cord thirty-one pairs of spinal nerves arise, each by an anterior and a posterior root (see NERVOUS SYSTEM). The cord is not of uniform circumference throughout. There is a slight thickening where the brachial nerves, and another where the lumbar nerves, arise. These are termed the brachial or cervical and lumbar enlargements respectively. The nerve roots in the cervical and dorsal regions pass nearly transversely outwards through the intervertebral foramina; but the lumbar and sacral nerves are directed downwards to attain their points of exit, in such a manner as to obtain the name of Cauda Equina.
The cord is seen to be composed of white and gray matter. On a transverse section the gray matter is found in the centre to present the appearance of a double crescent, concave outwards, with a commissural band between the two sides, so that the whole somewhat resembles the letter H. In the gray commissure is the central canal, which extends throughout the whole length of the cord and becomes continuous above with the fourth ventricle. The gray matter is divided into an anterior and a posterior horn. It is composed of a basis of connective tissue in which are a fine felt-work of nerve-fibres and nerve-cells. In the anterior horn, which becomes specially developed in the brachial and lumbar enlargements, the cells are of the multipolar type. They send a well-marked axis cylinder process into the anterior nerve root, and by their other processes are connected with fibres which descend from the cerebrum and from the posterior roots and other sources. In the posterior horn the nerve-cells are smaller, rounded, or spindle-shaped, and possess no axis cylinder process. They are probably connected with the posterior roots.
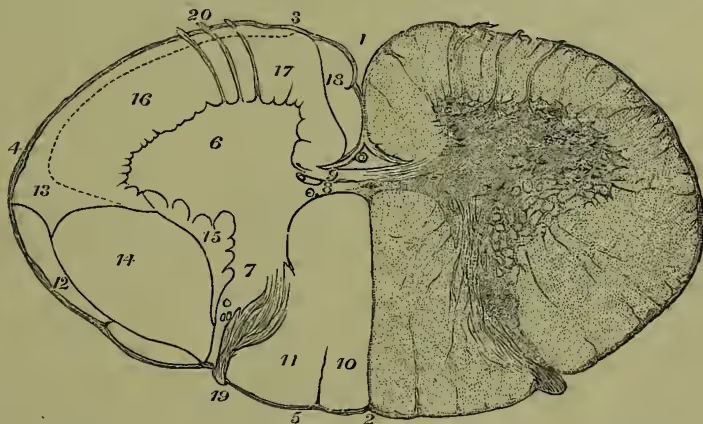
The white matter of the cord is composed of nerve-fibres, united by a small amount of connective tissue. The fibres have mostly a longitudinal direction, with the exception of a small strand which crosses from one side to the other at the bottom of the anterior median fissure—the anterior white commissure. Each half of the cord is divided by the anterior and posterior roots into three columns, named anterior, lateral, and posterior. Though these look almost exactly alike both to the naked eye and under the microscope, they can, by taking advantage of the facts that their component fibres are not all developed simultaneously, and that as the result of injury they do not 'degenerate' in the same direction or to the same extent, be further subdivided. Thus the posterior column is composed of two tracts—a postero-medial and a postero-lateral. In the lateral column there can be distinguished five tracts: a direct cerebellar, an ascending antero-lateral tract, a crossed pyramidal tract, a lateral limiting layer, and a lateral mixed zone; while the anterior column consists of a direct pyramidal tract and an anterior mixed zone. The relations of these tracts have been fairly definitely established. The postero-medial column is nearly entirely composed of fibres of the posterior roots which, after entering the cord and passing for a short distance in the postero-external column, are continued upwards as high as the medulla oblongata, where they end. This column then will form a direct path of connection of the posterior roots with the medulla oblongata. The direct cerebellar tract connects a column of nerve-cells in the posterior horn of the lumbar and dorsal regions of the cord (which is termed Clarke's vesicular column) with the middle lobe of the cerebellum. The antero-lateral tract appears to connect the nerve-cells in the posterior horn of one side of the cord with the medulla oblongata of the opposite side. 1, anterior median fissure; 2, posterior median septum; 3, 4, 5, anterior, lateral, and posterior white columns; 6, 7, anterior and posterior horn of gray matter; 8, 9, anterior and posterior commissures; 10, posterior median column; 11, posterior lateral column; 12, direct cerebellar tract; 13, antero-lateral ascending tract; 14, crossed pyramidal tract; 15, lateral limiting layer; 16, 17, lateral and anterior mixed zone; 18, anterior pyramidal tract; 19, posterior, and 20, anterior roots.
All these tracts degenerate, and presumably also conduct nervous impulses in an upward direction. The direct and crossed pyramidal tracts form the downward continuation of the 'motor'-fibres from the surface of the brain to the cells in the anterior cornu of the cord. At the lower end of the medulla oblongata (see BRAIN, fig. 7) the greater part of the fibres of the anterior pyramids cross the middle line and descend in the crossed pyramidal tract of the cord to become connected with the motor-cells in the anterior horn. The direct pyramidal tract represents a small remnant of the fibres which descend in the cord without crossing to the opposite side. They cannot as a rule be traced further than the cervical region. Both of these tracts are undoubtedly concerned in the transmission of voluntary motor impulses from the brain. Their degeneration always accompanies paralysis of cerebral origin.
The tracts which lie in immediate contact with the gray matter, the antero-lateral mixed zone, the lateral limiting layer, and the postero-external column, probably form connections between different levels of the cord. Thus the postero-external column is in great part formed of fibres of the posterior roots passing upwards or downwards for a certain distance in it before entering the postero-internal column; while the antero-lateral mixed zone contains fibres which connect either nerve-cells at different levels, or more probably nerve-cells of one level with fibres which enter the anterior roots at another.
Functions.—The spinal cord provides paths for the conduction of afferent and efferent impulses to and from the brain, and also between different portions of its own substance, as well as arrangements for co-ordination of movements of the muscles of the trunk and limbs, and centres for the regulation of certain of the 'organic' functions of the body.
The efferent impulses are motor, vasomotor, and secretory. The path for the first of these is perfectly well known. It passes from the cerebral cortex (motor area) through the internal capsule and the anterior pyramids of the medulla mainly to the crossed pyramidal tract of the opposite side, and thence, as described, to the cells in the anterior cornu. It is not yet known whether the ultimate destination of the fibres of the direct pyramidal tract is the cells of the anterior horn of the same or those of the opposite side. The fibres from the vasomotor centre in the medulla in all probability pass down in the crossed pyramidal tract and leave the cord by the anterior roots. Division of their path leads to paralysis of the muscular walls and dilatation of the arteries. This is only temporary, as there are probably also centres in the cord which can act independently of those in the medulla. The other efferent paths are unknown.
The afferent paths transmit the various forms of sensory impulses; but, though we may perhaps assume that those which degenerate upwards also conduct in the same direction, it is remarkable how little is known definitely about these. It is generally held that impulses from the muscles pass up the same side of the cord either in the postero-median or direct cerebellar tracts; while the other sensory paths cross the cord as soon as they enter it, and are continued upwards along the other side. It is not determined whether the crossing is complete, or whether the path is in the white or gray matter or in both. Probably it is not identical for each variety of sensation. There is some reason to believe that impulses which give rise to painful sensations travel up the ascending antero-lateral tract.
The cord also has in its anterior cornu cells which, when stimulated either from the brain or from the sensory nerves, originate voluntary or reflex muscular movements. These cells fulfil too the function of keeping up the general tone of the muscles and also their nutrition, for when they are destroyed the nerves and muscles connected with them waste and disappear. In certain regions of the cord these cells form centres for various of the organic functions. These are found mostly in the lower dorsal and lumbar regions. Recent experimental research by Ferrier and Yeo has determined the levels in the cord of the centres for the various movements of the limbs and trunk, and has already given valuable results in practical surgery.
See Quain's Anatomy, Obersteiner's Anatomy of the Central Nervous Organs (Hill's trans.), Landois and Stirling's Physiology, and Foster's Physiology.
CURVATURE OF THE SPINE.—There are two main forms of this disease, which are due to different causes—viz. Angular Curvature or Pott's Curvature, and Lateral Curvature.
Angular curvature, which was first described by the famous surgeon Percival Pott (1713-88), and is hence often named after him, is due to disease of the bodies of the vertebrae and of the intervertebral discs. It usually takes the form of a tubercular disease of the bones, which become carious and destroyed, and of ulceration of the discs between them. The result is that the bodies of the diseased vertebrae give way and the column becomes bent forward on itself, while the spinous processes form a backward projection opposite the diseased part—hence the name angular curvature. This projection is most marked when the disease is in the dorsal region of the spine. If the disease is arrested the bones become firmly united, and the curve of the spine becomes permanent. In unfavourable cases abscesses may develop in the neighbourhood, and either press on the spinal cord or on the spinal nerves, or burrow in various directions, notably in the lumbar region (psoas abscess). The disease is often set up by an injury which may be severe, such as the falling of a heavy weight on the back, or in children may be some trifling twist or fall, such as may occur during rough play or from falling out of bed or from a chair. It most often occurs in delicate children with a tubercular family history, but it is by no means unknown in those whose family and personal history is quite unexceptionable, and it may even affect adults. Its early symptoms are often obscure, and consequently may be overlooked at a time when treatment is of most avail. There is at first little or no deformity, but there may be pain on percussing the spine of the affected vertebrae. There is also usually an avoidance of all movements which may lead to jarring of the spinal column or to painful pressure on the nerves. If the vertebrae of the neck are affected the child often supports its chin by the hands, and does not willingly turn its head round. Disease of the dorsal or lumbar vertebrae is generally indicated by cautious movements, especially in coming down a stair, the avoidance of stooping or bending, or sudden twisting of the body. A child will thus get down on its knees to pick anything off the floor rather than stoop.
The treatment requires to be both local and constitutional. It is always protracted for months or even years. The general treatment is mainly that required for strumous constitutions, such as codliver-oil, iron, hypophosphate of lime, &c. The local treatment involves absolute rest in the recumbent position in the early stage, with counter irritation over the spine in the neighbourhood of the disease. In later stages mechanical supports are also required to keep the vertebrae from pressing on each other. The kind of support needed varies with the region affected; one very valuable form for hospital practice consists in the application, during the suspension of the patient, of a plaster of Paris jacket to the body. The more carefully rest in the recumbent position and mechanical support are carried out, the less, as a rule, will be the resulting deformity, the greater the prospect of avoiding complications and of obtaining permanent cure.
Lateral curvature consists in a twisting of the bodies of the vertebrae on each other round their vertical axis. It is sometimes a result of rickets, but is far more frequently developed in growing girls of feeble muscular development and general health, between the ages of ten and sixteen. It is produced in the first instance by the continued maintenance of asymmetrical positions of the body, such as by sitting sideways or cross-legged before a school-desk, or by carrying a weight on one arm. This curvature is usually to the right in the dorsal region with a corresponding twist to the left in the lumbar region. One shoulder, usually the right, becomes elevated, and the scapula projects, while the right side of the chest becomes rounded and the left side flattened. The lungs and liver become compressed and subject to disease, and the gait becomes awkward. This disease is due in the first instance to rotation of the bodies of the vertebrae on each other as the result of the irregular pressure. Later the ligaments and articular processes of the vertebrae undergo permanent changes, while the muscles may atrophy or undergo fatty degeneration. The ribs also become distorted, those at the side of the convexity of the curve bending at the angles, those at the other side becoming flattened.
The treatment of this form differs entirely from that of angular curvature. As the disease is due to the continuance of asymmetrical positions of the body, combined with muscular and general debility, general tonics, fresh air, and gymnastic exercise specially directed to the strengthening of the weakened muscles must be adopted. In the later stages, when the deformity has become more confirmed, mechanical supports may be required as an adjuvant to the above.